

Efficacy and safety of femoral nerve block for the positioning of femur fracture patients before a spinal block - A systematic review and meta-analysis
- PMID: 31048897
- PMCID: PMC6497313
- DOI: 10.1371/journal.pone.0216337
Efficacy and safety of femoral nerve block for the positioning of femur fracture patients before a spinal block - A systematic review and meta-analysis
Abstract
Background: The evidence supporting the benefit of femoral nerve block (FNB) for positioning before spinal anesthesia (SA) in patients suffering from a femur fracture remains inconclusive. In the present study, the authors intended to determine the efficacy and safety of FNB versus an intravenous analgesic (IVA) for positioning before SA in patients with a femur fracture.
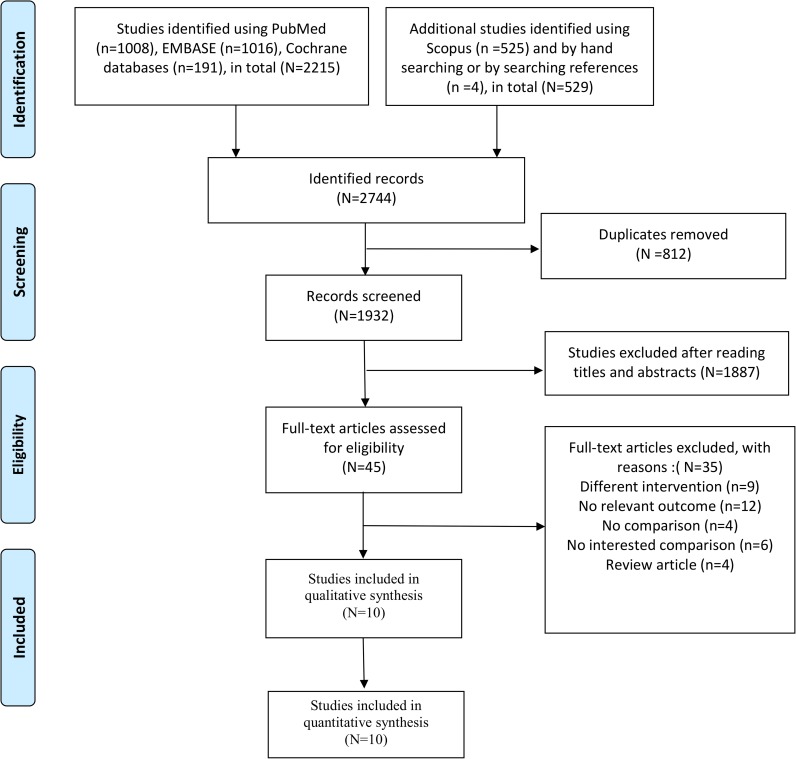
Method: PubMed, EMBASE, Cochrane, and Scopus databases were searched up to January 2018. We included randomized controlled studies (RCTs) and observational studies that compared FNB versus IVA for the positioning of patients with femur fracture receiving SA. The primary outcome was pain scores during positioning within 30 min before SA. Secondary outcomes were the time for SA, additional analgesic requirements, anesthesiologist's satisfaction with the quality of positioning for SA, participant acceptance, and hemodynamic changes. A random-effects model was used to synthesize the data. We registered the study at PROSPERO with an ID of CRD42018091450.
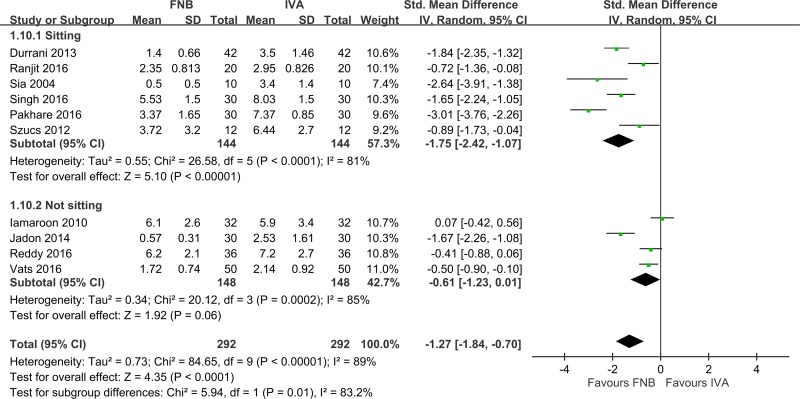
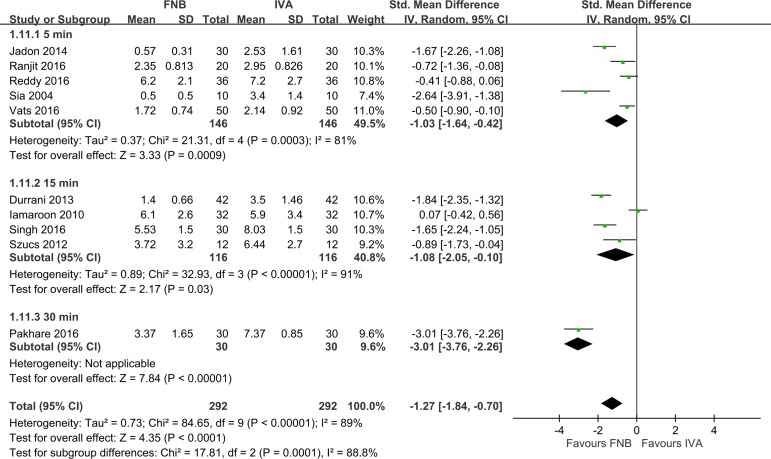
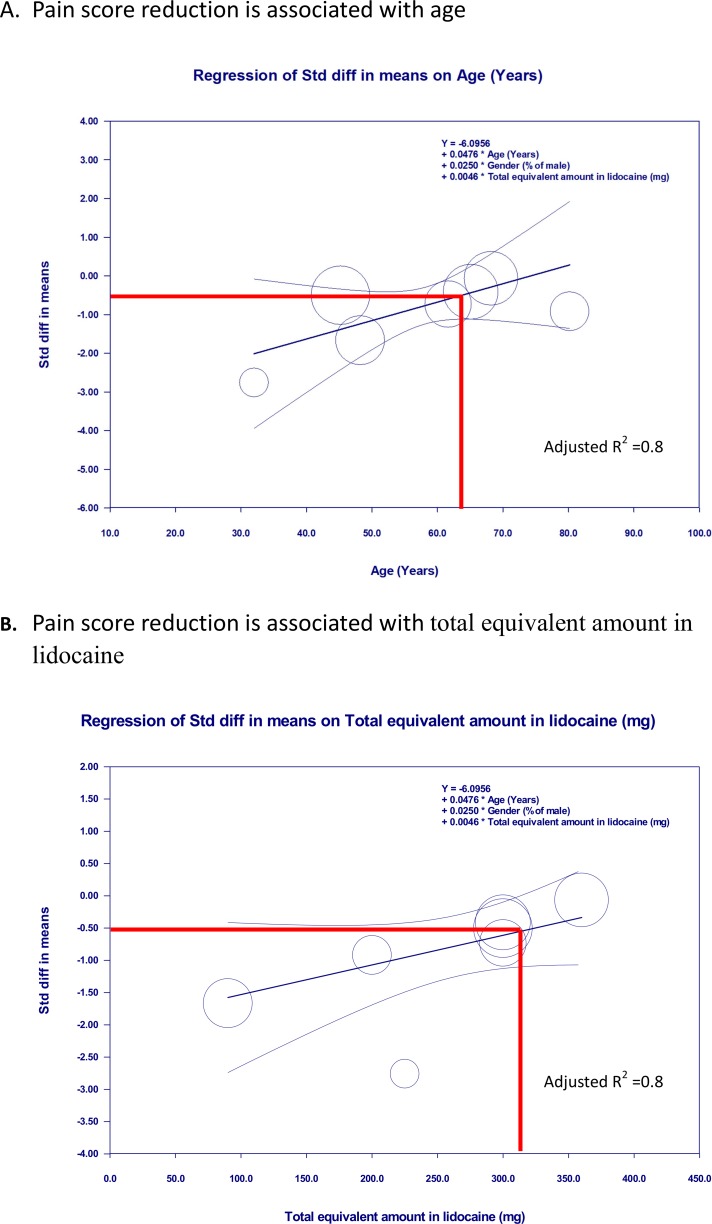
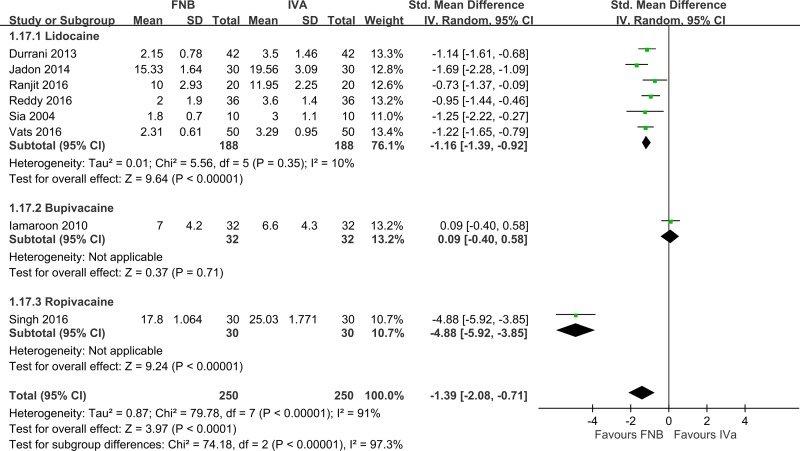
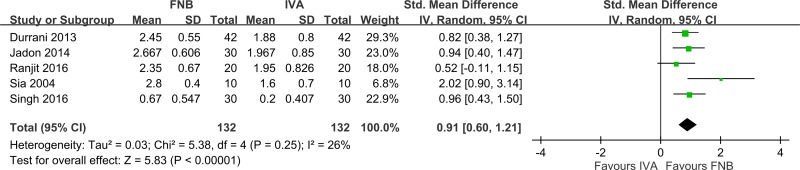
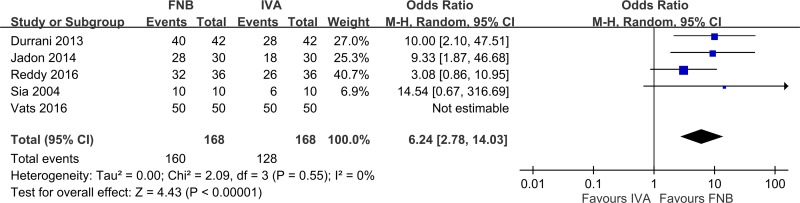
Results: Ten studies with 584 patients were eligible for inclusion. FNB achieved significantly lower pain scores than IVA during positioning within 30 min before SA (pooled standardized mean deviation (SMD): -1.27, 95% confidence interval (CI): -1.84 to -0.70, p < 0.05). A subgroup analysis showed that the analgesic effect was larger in patients in the sitting position for SA than a non-sitting position (sitting position vs non-sitting: pooled SMD: -1.75 (p < 0.05) vs -0.61 (not significant). A multivariate regression showed that the analgesic effect was also associated with age and the total equivalent amount as lidocaine after adjusting for gender (age: coefficient 0.048, p < 0.05; total equivalent amount as lidocaine: coefficient 0.005, p < 0.05). Patients receiving FNB also had a significantly shorter time for SA, greater anesthesiologist satisfaction, and higher patient acceptance than patients receiving IVA. The use of local anesthetics did not produce significant clinical hemodynamic change.
Conclusion: Compared to IVA, FNB was an effective and safe strategy for the positioning of femur fracture patients for a spinal block, particularly patients who received SA in the sitting position.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Koval KJ, Zuckerman JD. Hip Fractures: I. Overview and evaluation and treatment of femoral-neck fractures. J Am Acad Orthop Surg. 1994; 2: 141–9. - PubMed
-
- Maxwell L, White S. Anaesthetic management of patients with hip fractures: an update. Contin Educ Anaesth Crit Care Pain. 2013; 13: 179–83.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
