

Single-institution retrospective review of patients with recurrent glioblastoma treated with bevacizumab in clinical practice
- PMID: 31049419
- PMCID: PMC6482327
- DOI: 10.1002/hsr2.114
Single-institution retrospective review of patients with recurrent glioblastoma treated with bevacizumab in clinical practice
Abstract
Background and aims: This retrospective review of patients with recurrent glioblastoma treated at the Preston Robert Tisch Brain Tumor Center investigated treatment patterns, survival, and safety with bevacizumab in a real-world setting.
Methods: Adult patients with glioblastoma who initiated bevacizumab at disease progression between January 1, 2009, and May 14, 2012, were included. A Kaplan-Meier estimator was used to describe overall survival (OS), progression-free survival (PFS), and time to greater than or equal to 20% reduction in Karnofsky Performance Status (KPS). The effect of baseline demographic and clinical factors on survival was examined using a Cox proportional hazards model. Adverse event (AE) data were collected.
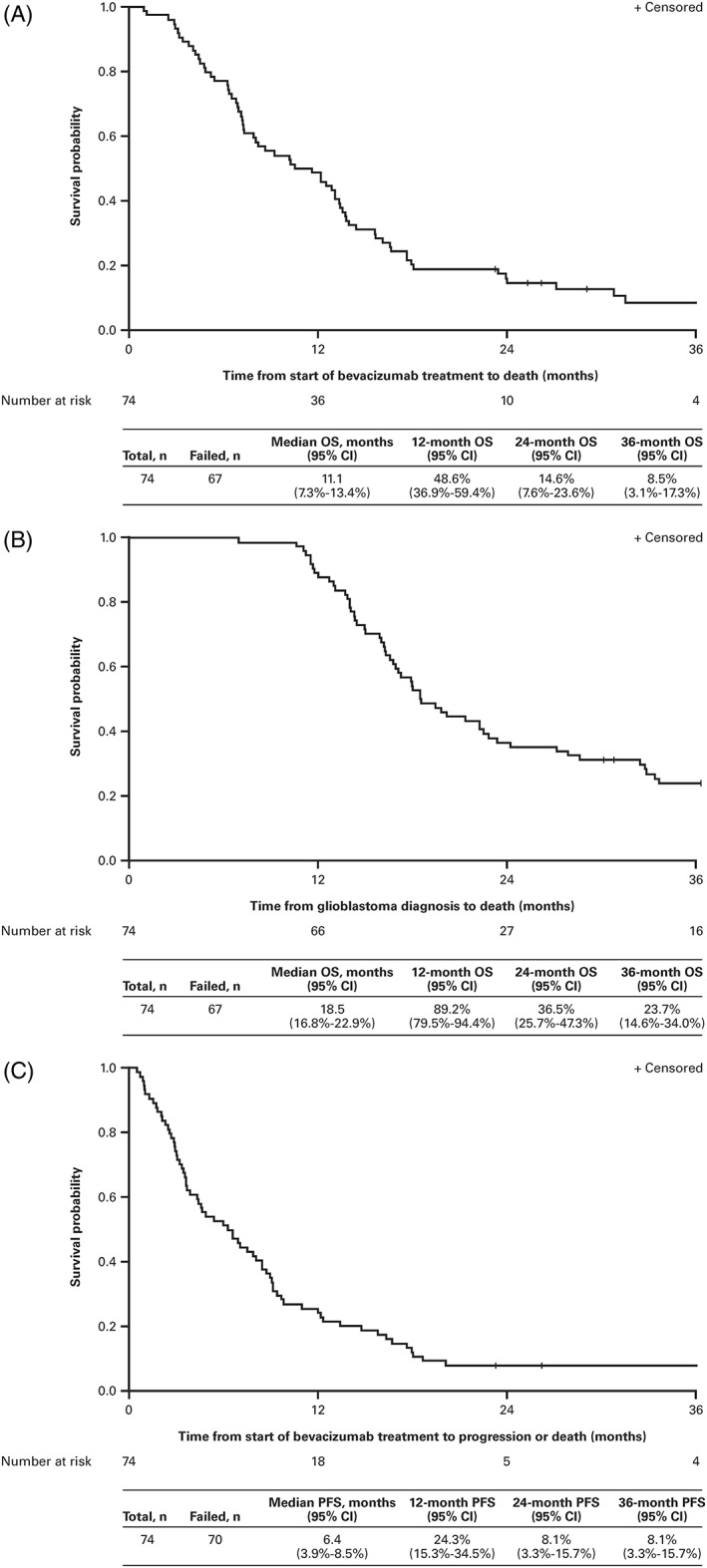
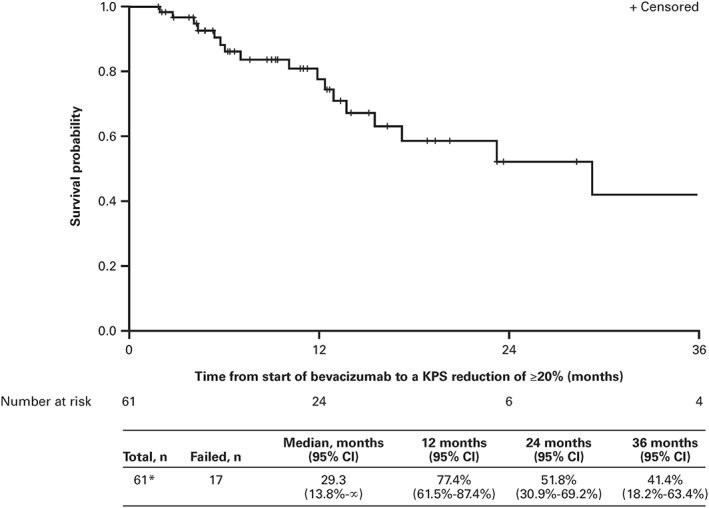
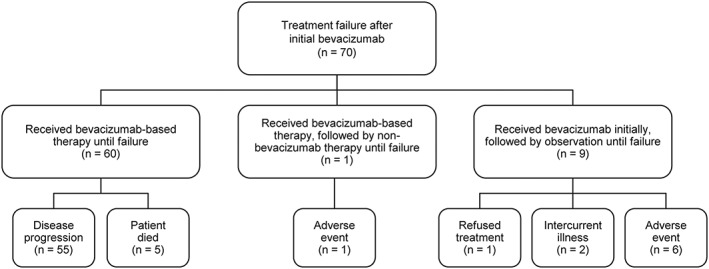
Results: Seventy-four patients, with a median age of 59 years, were included in this cohort. Between bevacizumab initiation and first failure, defined as the first disease progression after bevacizumab initiation, biweekly bevacizumab and bevacizumab/irinotecan were the most frequently prescribed regimens. Median duration of bevacizumab treatment until failure was 6.4 months (range, 0.5-58.7). Median OS and PFS from bevacizumab initiation were 11.1 months (95% confidence interval [CI], 7.3-13.4) and 6.4 months (95% CI, 3.9-8.5), respectively. Median time to greater than or equal to 20% reduction in KPS was 29.3 months (95% CI, 13.8-∞). Lack of corticosteroid usage at the start of bevacizumab therapy was associated with both longer OS and PFS, with a median OS of 13.2 months (95% CI, 8.6-16.6) in patients who did not initially require corticosteroids versus 7.2 months (95% CI, 4.8-12.5) in those who did (P = 0.0382, log-rank), while median PFS values were 8.6 months (95% CI, 4.6-9.7) and 3.7 months (95% CI, 2.7-6.6), respectively (P = 0.0243, log-rank). Treatment failure occurred in 70 patients; 47 of whom received salvage therapy, and most frequently bevacizumab/carboplatin (7/47; 14.9%). Thirteen patients (18%) experienced a grade 3 AE of special interest for bevacizumab.
Conclusions: Treatment patterns and outcomes for patients with recurrent glioblastoma receiving bevacizumab in a real-world setting were comparable with those reported in prospective clinical trials.
Keywords: bevacizumab; real‐world setting; recurrent glioblastoma; survival; treatment patterns.
Conflict of interest statement
Annick Desjardins has received grants or research support from Genentech, PTC Therapeutics, Celldex, Triphase Research and Development Corp, Eli Lilly and Co, Eisai, Symphogen A/S, Pfizer, and Orbus Therapeutic and is an advisory board member for Genentech; Arliene Ravelo is an employee of Genentech and owns stock options in Roche; Nicolas Sommer is an employee of Genentech and owns stock options in Roche; and the remaining authors have no conflicts of interest to declare.
Figures
References
-
- Ohgaki H, Dessen P, Jourde B, et al. Genetic pathways to glioblastoma: a population‐based study. Cancer Res. 2004;64(19):6892‐6899. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol. 1999;17(8):2572‐2578. - PubMed
-
- Lamszus K, Ulbricht U, Matschke J, Brockmann MA, Fillbrandt R, Westphal M. Levels of soluble vascular endothelial growth factor (VEGF) receptor 1 in astrocytic tumors and its relation to malignancy, vascularity, and VEGF‐A. Clin Cancer Res. 2003;9(4):1399‐1405. - PubMed
LinkOut - more resources
Full Text Sources
