

Epidemiology of Anaphylaxis in Critically Ill Children in the United States and Canada
- PMID: 31051271
- PMCID: PMC8411990
- DOI: 10.1016/j.jaip.2019.04.025
Epidemiology of Anaphylaxis in Critically Ill Children in the United States and Canada
Abstract
Background: Anaphylaxis is a rapid-onset, multisystem, and potentially fatal hypersensitivity reaction with varied reports of prevalence, incidence, and mortality. There are limited cases reported of severe and/or fatal pediatric anaphylaxis.
Objective: This study describes the largest cohort of intensive care unit pediatric anaphylaxis admissions with a comprehensive analysis of identified triggers, clinical and demographic information, and probability of death.
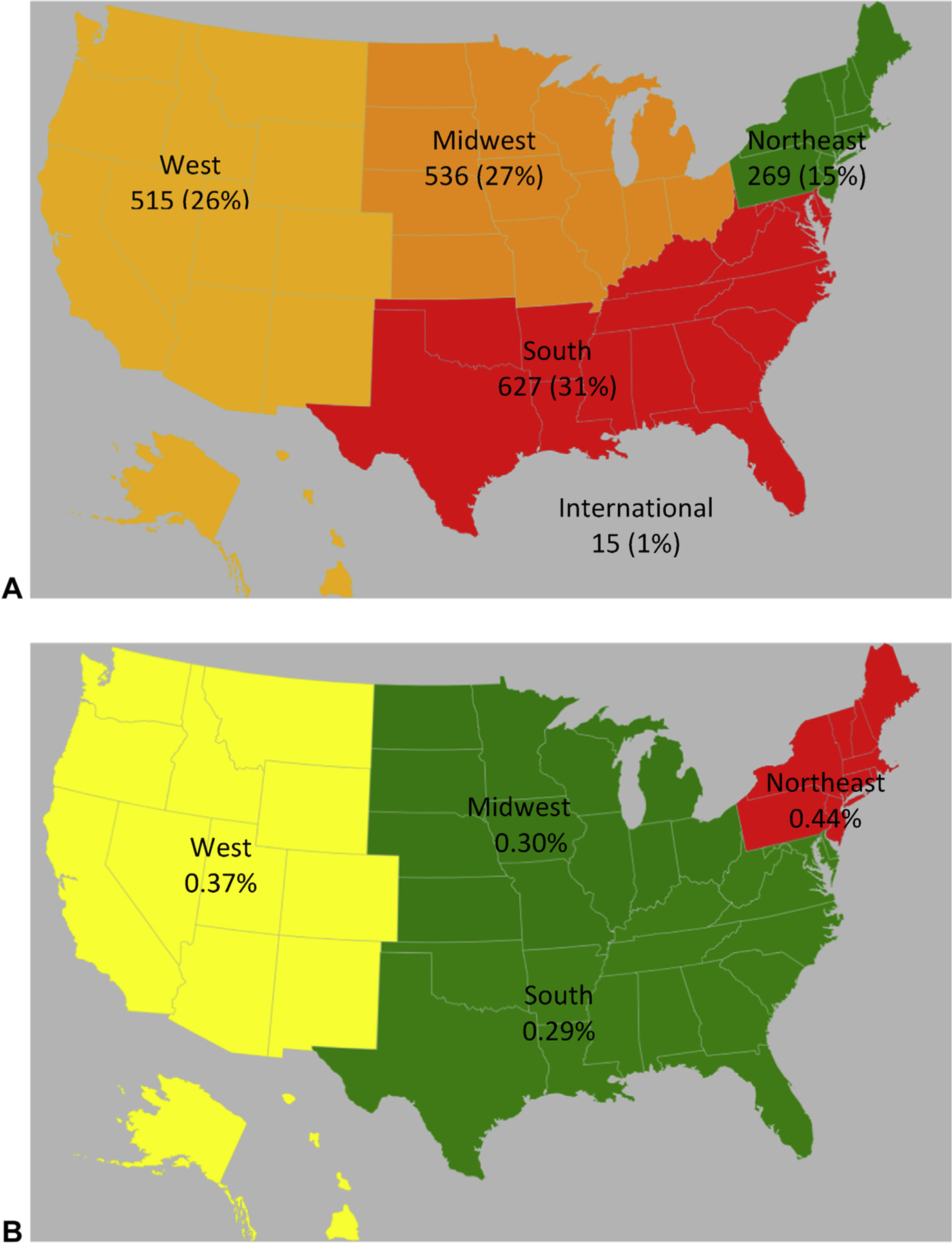
Methods: We describe the epidemiology of pediatric anaphylaxis admissions to North American pediatric intensive care units (PICUs) that were prospectively enrolled in the Virtual Pediatric Systems database from 2010 to 2015. One hundred thirty-one PICUs in North America (United States and Canada) were queried for anaphylaxis International Classification of Diseases, Ninth Revision or International Classification of Diseases, Tenth Revision codes from the Virtual Pediatric Systems database from 2010 to 2015 in the United States and Canada. One thousand nine hundred eighty-nine patients younger than 18 years were identified out of 604,279 total number of patients admitted to a PICU in the database during this time frame.
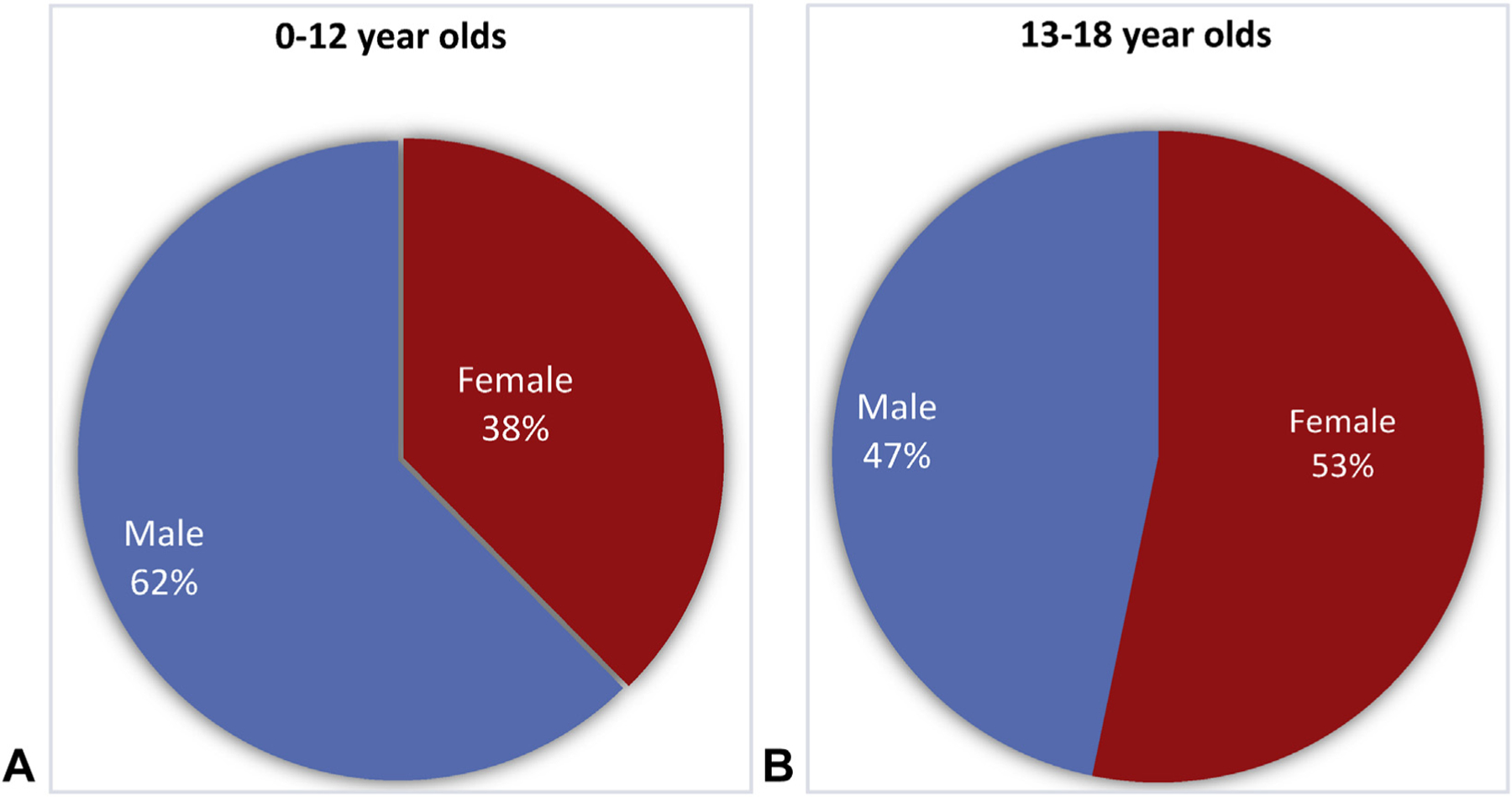
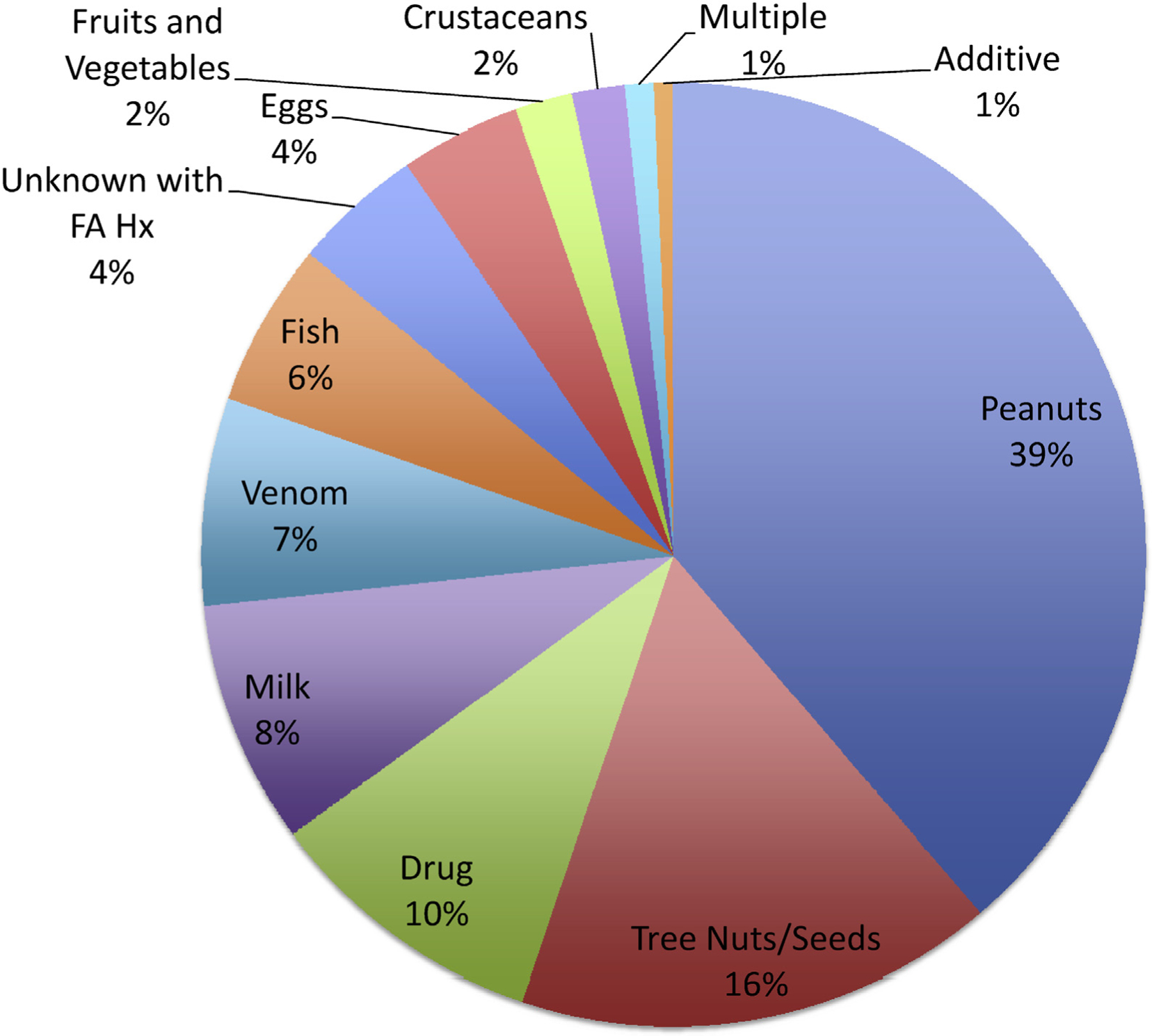
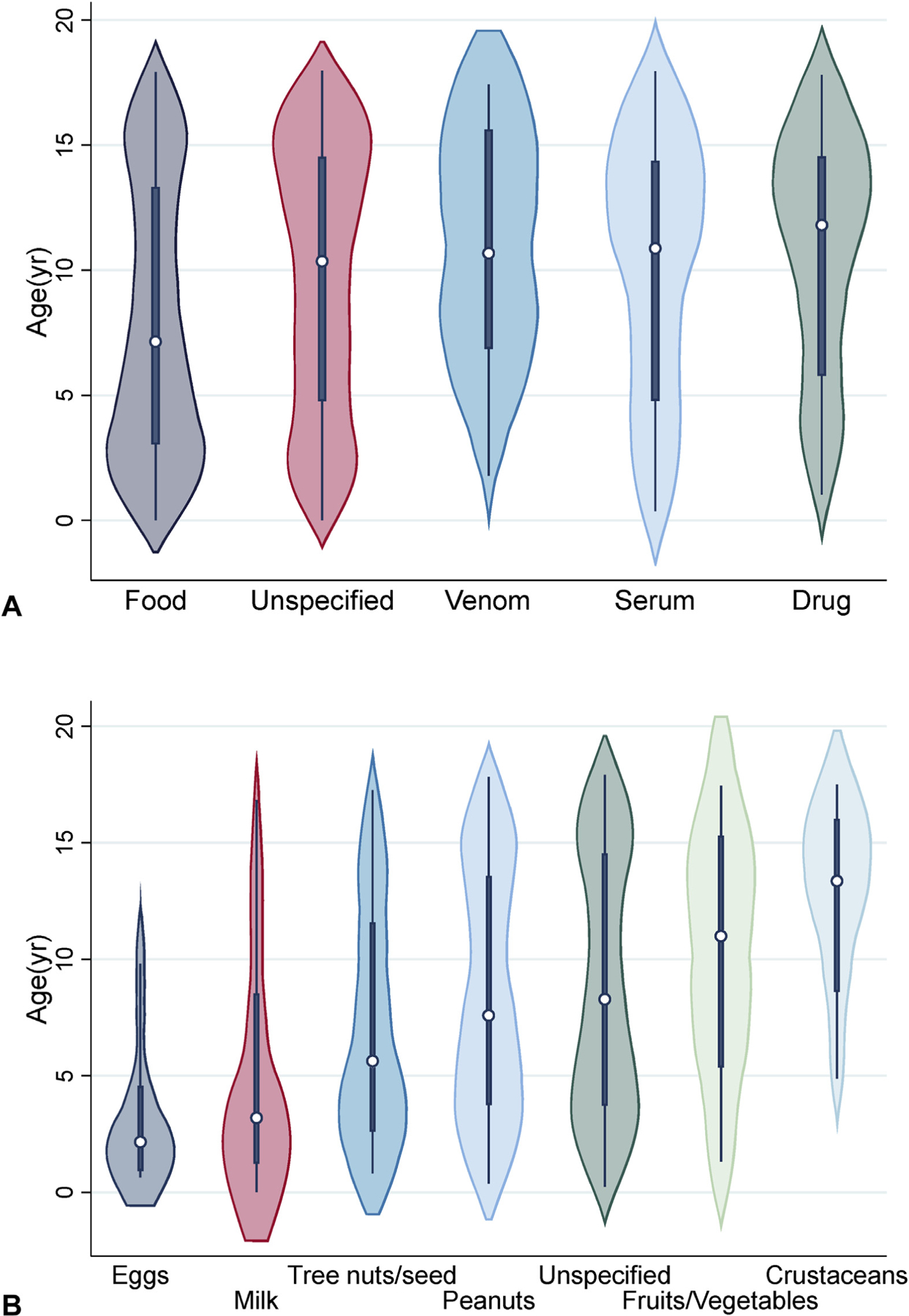
Results: The primary outcome was mortality, which was compared with patient and admission data using Fisher exact test. Secondary outcomes (intubation, length of stay, mortality risk scores, systolic blood pressure, and pupillary reflex) were analyzed using the Kruskal-Wallis test or Wilcoxon rank-sum test, as appropriate. One thousand nine hundred eighty-nine patients with an anaphylaxis International Classification of Diseases code were identified in the database. One percent of patients died because of critical anaphylaxis. Identified triggers for fatal cases were peanuts, milk, and blood products. Peanuts were the most common trigger. Children were mostly male when younger than 13 years, and mostly female when 13 years and older. Average length of stay was 2 days. There was a higher proportion of Asian patients younger than 2 years or when the trigger was food.
Conclusions: This is the largest study to describe pediatric critical anaphylaxis cases in North America and identifies food as the most common trigger. Death occurs in 1% of cases, with intubation occurring most commonly in the first hour. The risk for intensive care unit admission in children underscores the serious nature of anaphylaxis in this population.
Keywords: Adolescent; Anaphylaxis; Critically ill; ICU; Milk; Mortality; Peanut; Pediatric.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Most Children and Adolescents Will Survive an Episode of Severe Anaphylaxis, But We Need to Be Better at Prevention, Risk Reduction, and Early Treatment.J Allergy Clin Immunol Pract. 2019 Sep-Oct;7(7):2250-2251. doi: 10.1016/j.jaip.2019.06.013. J Allergy Clin Immunol Pract. 2019. PMID: 31495430 No abstract available.
References
-
- Tejedor Alonso MA, Moro Moro M, Múgica García MV. Epidemiology of anaphylaxis. Clin Exp Allergy 2015;45:1027–39. - PubMed
-
- Yu JE, Lin RY. The epidemiology of anaphylaxis. Clin Rev Allergy Immunol. Available from: http://link.springer.com/10.1007/s12016-015-8503-x.AccessedMarch 1, 2018. - DOI - PubMed
-
- Bohlke K, Davis RL, DeStefano F, Marcy SM, Braun MM, Thompson RS, et al.Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization. J Allergy Clin Immunol 2004;113:536–42. - PubMed
-
- Simon MR, Mulla ZD. A population-based epidemiologic analysis of deaths from anaphylaxis in Florida. Allergy 2008;63:1077–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
