

Heterogeneity of treatment effect by baseline risk of mortality in critically ill patients: re-analysis of three recent sepsis and ARDS randomised controlled trials
- PMID: 31053084
- PMCID: PMC6500045
- DOI: 10.1186/s13054-019-2446-1
Heterogeneity of treatment effect by baseline risk of mortality in critically ill patients: re-analysis of three recent sepsis and ARDS randomised controlled trials
Abstract
Background: Randomised controlled trials (RCTs) enrolling patients with sepsis or acute respiratory distress syndrome (ARDS) generate heterogeneous trial populations. Non-random variation in the treatment effect of an intervention due to differences in the baseline risk of death between patients in a population represents one form of heterogeneity of treatment effect (HTE). We assessed whether HTE in two sepsis and one ARDS RCTs could explain indeterminate trial results and inform future trial design.
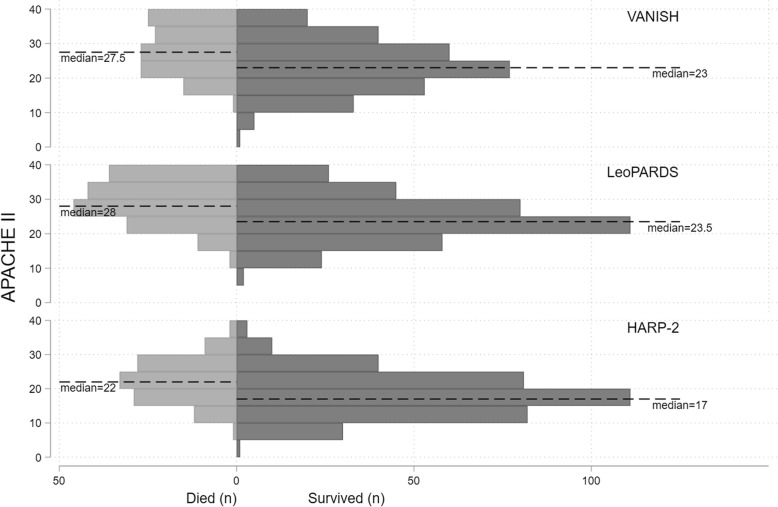
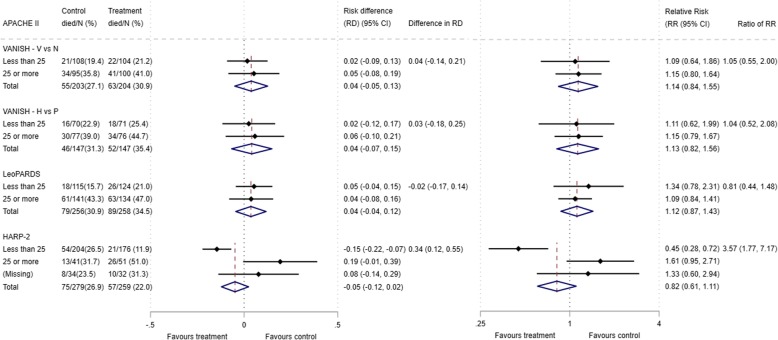
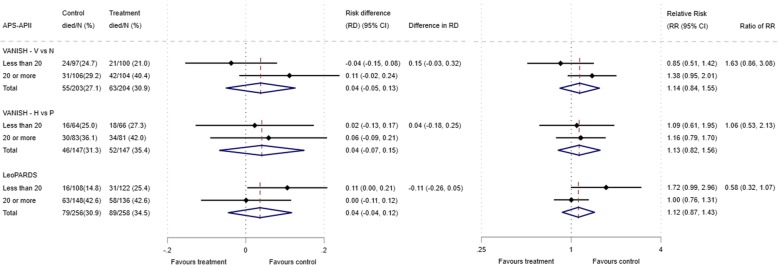
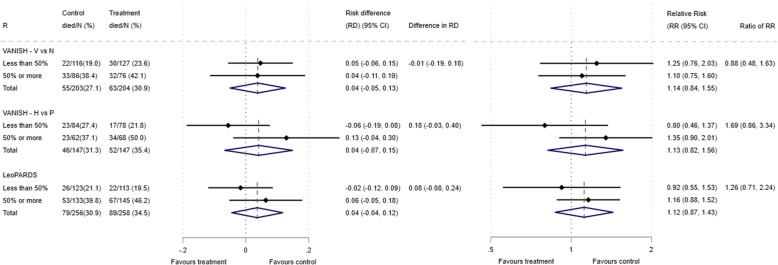
Methods: We assessed HTE for vasopressin, hydrocortisone and levosimendan in sepsis and simvastatin in ARDS patients, on 28-day mortality, using the total Acute Physiology And Chronic Health Evaluation II (APACHE II) score as the baseline risk measurement, comparing above (high) and below (low) the median score. Secondary risk measures were the acute physiology component of APACHE II and predicted risk of mortality using the APACHE II score. HTE was quantified both in additive (difference in risk difference (RD)) and multiplicative (ratio of relative risks (RR)) scales using estimated treatment differences from a logistic regression model with treatment risk as the interaction term.
Results: The ratio of the odds of death in the highest APACHE II quartile was 4.9 to 7.4 times compared to the lowest quartile, across the three trials. We did not observe HTE for vasopressin, hydrocortisone and levosimendan in the two sepsis trials. In the HARP-2 trial, simvastatin reduced mortality in the low APACHE II group and increased mortality in the high APACHE II group (difference in RD = 0.34 (0.12, 0.55) (p = 0.02); ratio of RR 3.57 (1.77, 7.17) (p < 0.001). The HTE patterns were inconsistent across the secondary risk measures. The sensitivity analyses of HTE effects for vasopressin, hydrocortisone and levosimendan were consistent with the main analyses and attenuated for simvastatin.
Conclusions: We assessed HTE in three recent ICU RCTs, using multivariable baseline risk of death models. There was considerable within-trial variation in the baseline risk of death. We observed potential HTE for simvastatin in ARDS, but no evidence of HTE for vasopressin, hydrocortisone or levosimendan in the two sepsis trials. Our findings could be explained either by true lack of HTE (no benefit of vasopressin, hydrocortisone or levosimendan vs comparator for any patient subgroups) or by lack of power to detect HTE. Our results require validation using similar trial databases.
Keywords: Models, statistical; Randomisation; Risk; Sepsis, acute respiratory distress syndrome; Study design.
Conflict of interest statement
Ethics approval and consent to participate
We obtained ethics approval for this study (18/LO/1079).
Consent for publication
We obtained consent to publish non-identifiable data.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. - PubMed
-
- Scicluna BP, van Vught LA, Zwinderman AH, Wiewel MA, Davenport EE, Burnham KL, Nurnberg P, Schultz MJ, Horn J, Cremer OL, et al. Classification of patients with sepsis according to blood genomic endotype: a prospective cohort study. Lancet Respir Med. 2017;5(10):816–826. doi: 10.1016/S2213-2600(17)30294-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- EME/16/33/01/DH_/Department of Health/United Kingdom
- MC_G1002460/MRC_/Medical Research Council/United Kingdom
- NIHR-CS-2016-16-011/Research Trainees Coordinating Centre/International
- MC_PC_13093/MRC_/Medical Research Council/United Kingdom
- RP-2015-06-018/Research Trainees Coordinating Centre/International
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
