

Identifying musculoskeletal conditions in electronic medical records: a prevalence and validation study using the Deliver Primary Healthcare Information (DELPHI) database
- PMID: 31053119
- PMCID: PMC6499985
- DOI: 10.1186/s12891-019-2568-2
Identifying musculoskeletal conditions in electronic medical records: a prevalence and validation study using the Deliver Primary Healthcare Information (DELPHI) database
Abstract
Background: Musculoskeletal (MSK) conditions are a common presentation in primary care. This study sought to determine the prevalence of MSK conditions in primary care in Ontario and to validate the extent to which health administrative date billing codes accurately represent MSK diagnoses.
Methods: De-identified electronic medical records (EMR) from the DELPHI database in southwestern Ontario, which contains 2493 patients (55.6% female, mean age 50.3 years (SD = 22.2)) and 21,964 encounters (July 1, 2006-June 30, 2010) were used for the analyses. Outcomes included: validation measures of agreement between International Classification of Diseases (ICD-9) diagnostic codes (health administrative data) and International Classification of Primary Care (ICPC) diagnoses defined as the reference standard, time to first ICD-9 code, prevalence, and healthcare utilization.
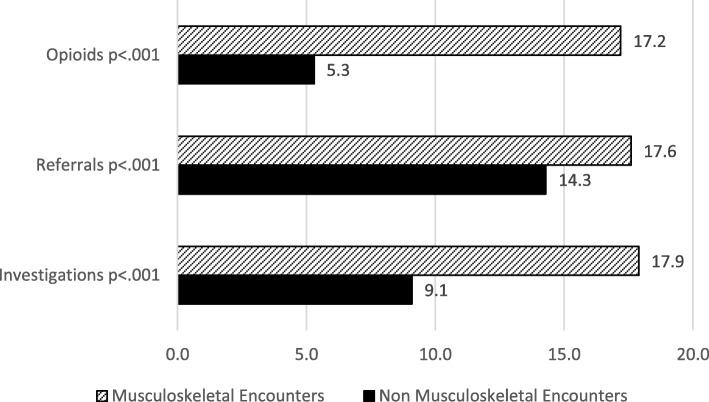
Results: There were 2940 true positive MSK encounters with primary care practitioners for 998 patients. Performance of the ICD-9 diagnostic codes included sensitivity = 76.5%, specificity = 95.2%, PPV = 94.6%, and NPV = 78.7%, compared to the ICPC reference standard. The majority of 998 patients were coded with both an ICPC and ICD-9 MSK code at their first or second encounter (67.4%). However, 23.5% of patients with the ICPC reference standard MSK were never coded with ICD-9. Four-year prevalence of MSK was 52.3% and varied by age (4.5% 0-17 years, 20.1% 18-44, 42.7% 45-64, and 32.7% 65+). Patients at MSK encounters had a higher number of: investigations (17.9% compared to 9.1%, p < .0001); referrals (17.6% compared to 14.3%, p < .0001); and prescriptions for opioids (17.2% compared to 5.3%, p < .0001).
Conclusions: This study determined the prevalence of musculoskeletal conditions in primary care in Ontario using a reference standard definition. The study highlighted the value of using primary care ICPC codes to validate a definition for musculoskeletal conditions. Health administrative data can be used to ascertain the presence of musculoskeletal conditions; however, ICD-9 codes may underrepresent the prevalence of MSK conditions.
Keywords: DELPHI database; Electronic medical records; Health administrative data; International classification of diseases; International classification of primary care; Musculoskeletal conditions; Validation.
Conflict of interest statement
Ethics approval and consent to participate
The DELPHI study received approval from The University of Western Ontario’s Review Board for Health Sciences Research Involving Human Subjects (#11151E). Written consent was obtained from all physician participants in the DELPHI project. The physicians are the data custodians of the patient’s EMR.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- MacKay C, Canizares M, Davis A, Badley E. Health care utilization for musculoskeletal disorders. Arthritis Care Res. 2010;62:161–169. - PubMed
-
- Croft P, Peat G, Van Der Windt D. Primary care research and musculoskeletal medicine. Prim Health Care Res Dev. 2009;11:4–16. doi: 10.1017/S1463423609990272. - DOI
-
- Statistics Canada Canadian Community Health Survey – Annual Component (CCHS): Detailed Information for 2012. http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&Id=135927. Accessed 9 Aug 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
