

Lifetime Occurrence of Brain Metastases Arising from Lung, Breast, and Skin Cancers in the Elderly: A SEER-Medicare Study
- PMID: 31053636
- PMCID: PMC6506177
- DOI: 10.1158/1055-9965.EPI-18-1116
Lifetime Occurrence of Brain Metastases Arising from Lung, Breast, and Skin Cancers in the Elderly: A SEER-Medicare Study
Abstract
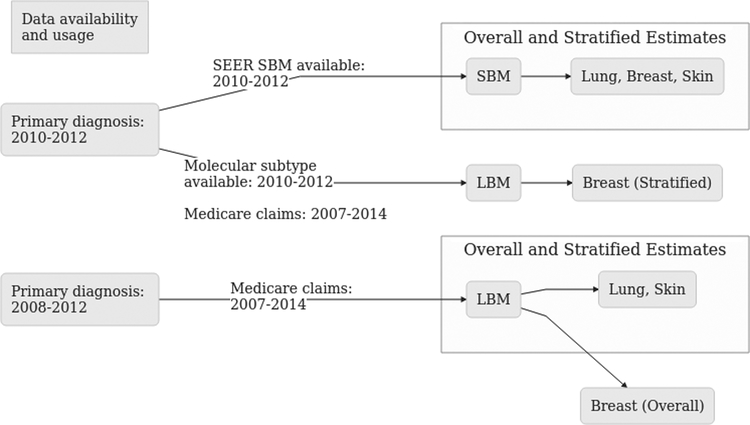
Background: The Surveillance, Epidemiology, and End Results (SEER) Program recently released data on brain metastases (BM) diagnosed during primary cancer staging workup ("synchronous" BM, or SBM); this study examines the incidence of SBM compared with that of lifetime BM (LBM) identified using Medicare claims for patients diagnosed with lung cancer, breast cancer, or melanoma.
Methods: Incidence proportions (IP) and age-adjusted rates for each of SEER SBM and Medicare LBM are presented along with measures of concordance between the two sources of data, where Medicare LBM were defined by several combinations of diagnosis and putative diagnostic imaging procedure codes.
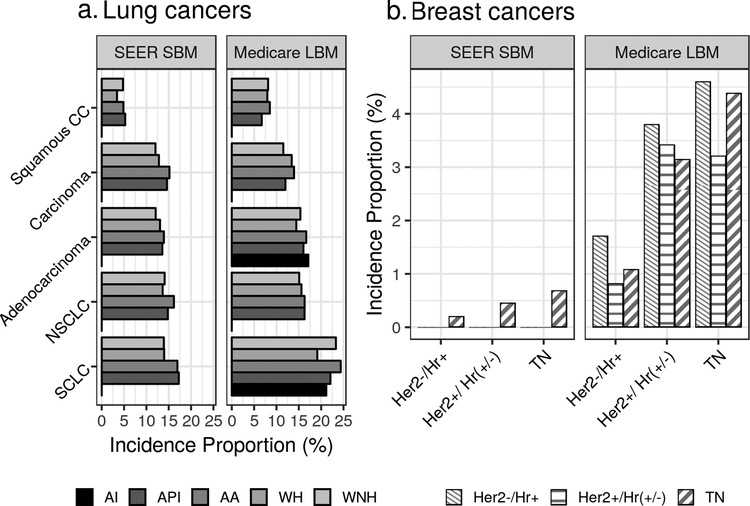
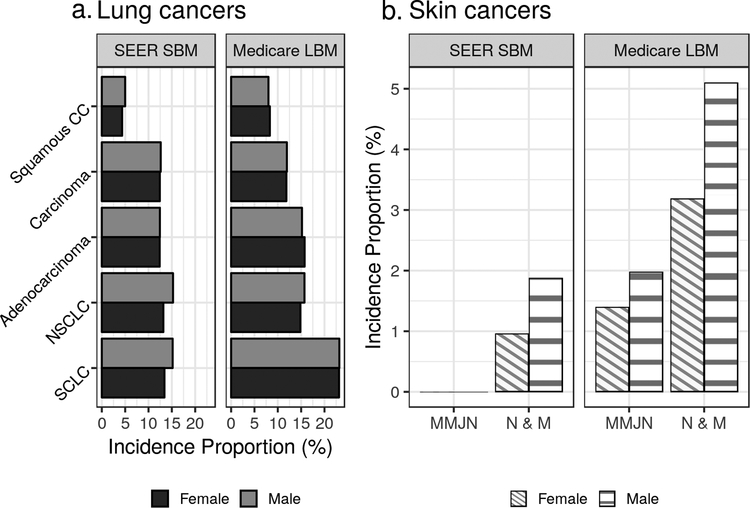
Results: The SBM IP in lung, breast, and melanoma cancers were 9.6%, 0.3%, and 1.1%, respectively; the corresponding LBM IP were 13.5%, 1.8%, and 3.6%. The greatest SBM IP among patients with lung cancer was 13.4% for non-small cell lung cancer, and among patients with breast cancer was 0.7% for triple-negative breast cancer. The greatest LBM IP among lung cancers was 23.1% in small-cell lung cancer, and among breast cancers was 4.2% for cases of the triple negative subtype.
Conclusions: Using a large dataset that is representative of the elderly population in the United States, these analyses estimate synchronous and lifetime incidence of BM in lung cancers, breast cancers, and melanomas.
Impact: These and other population-based estimates may be used to guide development of BM screening policy and evaluation of real-world data sources.
©2019 American Association for Cancer Research.
Conflict of interest statement
Conflicts of Interest
The author Mustafa S Ascha has no potential conflicts of interest to disclose.
The author Quinn T Ostrom has no potential conflicts of interest to disclose.
The author James Wright has no potential conflicts of interest to disclose.
The author Priya Kumthekar has no potential conflicts of interest to disclose.
The author Jeremy S Bordeaux has no potential conflicts of interest to disclose.
The author Andrew E Sloan has no potential conflicts of interest to disclose.
The author Fredrick R Schumacher has no potential conflicts of interest to disclose.
The author Carol Kruchko has no potential conflicts of interest to disclose.
The author Jill S Barnholtz-Sloan has no potential conflicts of interest to disclose.
Figures
Comment in
-
Some elderly survivors of 3 common cancers have an increased risk of brain metastases.Cancer. 2019 Oct 1;125(19):3286-3287. doi: 10.1002/cncr.32493. Cancer. 2019. PMID: 31518006 No abstract available.
References
-
- Werner CA The older population: 2010. 2010 census briefs. document c2010br-09. 2011.
-
- Loeffler JS, Wen PY. Epidemiology, Clinical Manifestations, and Diagnosis of Brain Metastases. (DeAngelis LM, Eichler AF, eds.). Wolters Kluwer Health, UpToDate; 2018.
-
- Collaborative Stage Data Collection System User Documentation and Coding Instructions Version 02.03.02. Chicago, Illinois, United States of America: Collaborative Stage Work Group of the American Joint Committee on Cancer; American Joint Committee on Cancer; 2017.
-
- Kromer C, Xu J, Ostrom QT, et al. Estimating the annual frequency of synchronous brain metastasis in the united states 2010–2013: A population-based study. Journal of Neuro-Oncology. 2017:1–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
