

A longitudinal characterization of the Non-Cystic Fibrosis Bronchiectasis airway microbiome
- PMID: 31053725
- PMCID: PMC6499777
- DOI: 10.1038/s41598-019-42862-y
A longitudinal characterization of the Non-Cystic Fibrosis Bronchiectasis airway microbiome
Abstract
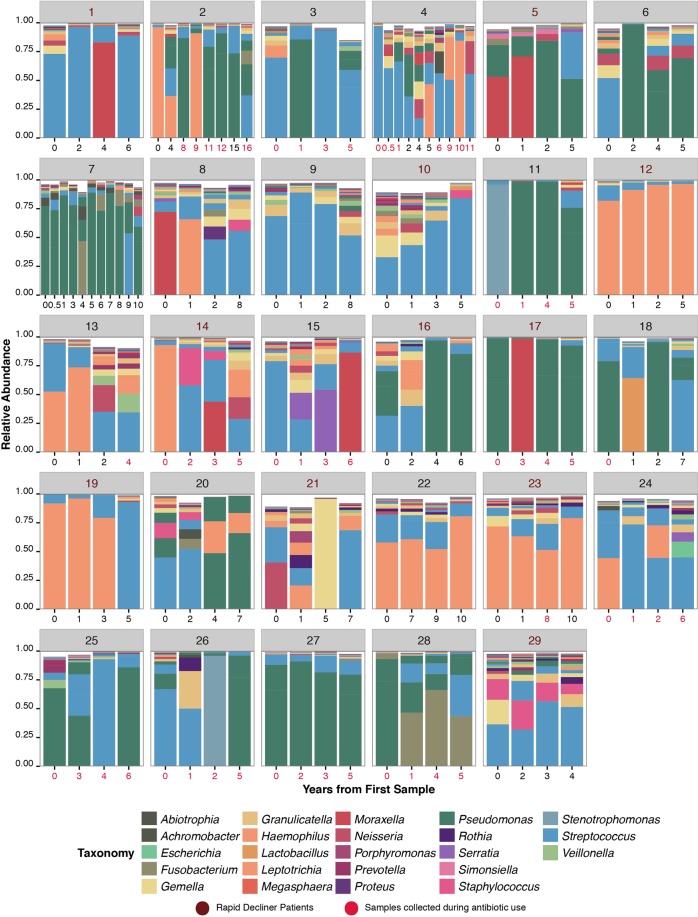
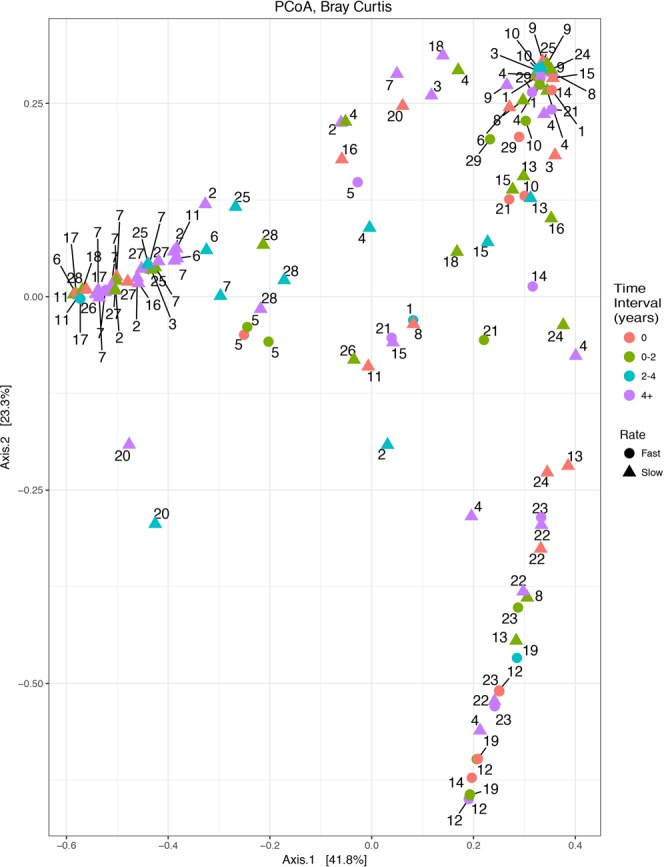
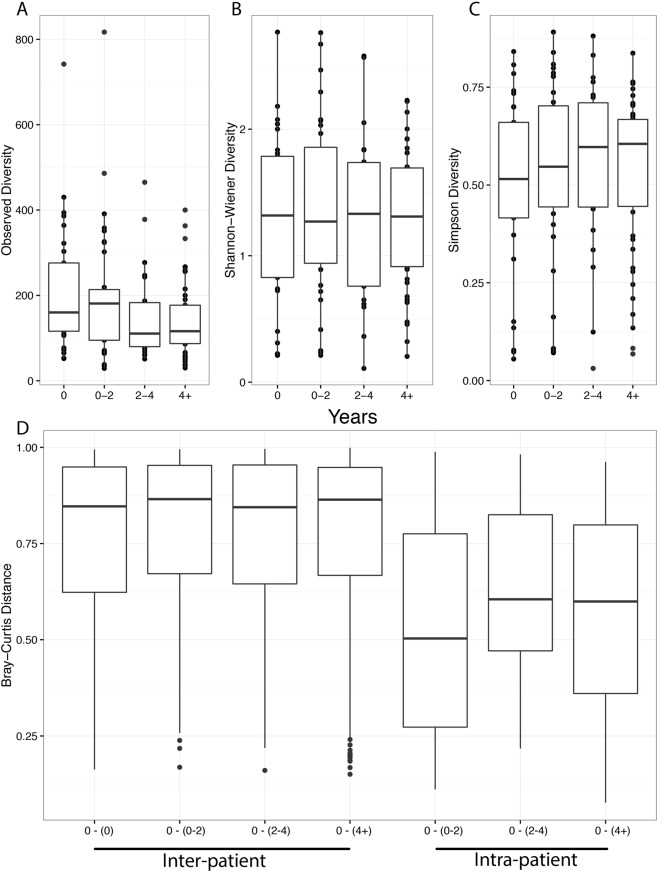
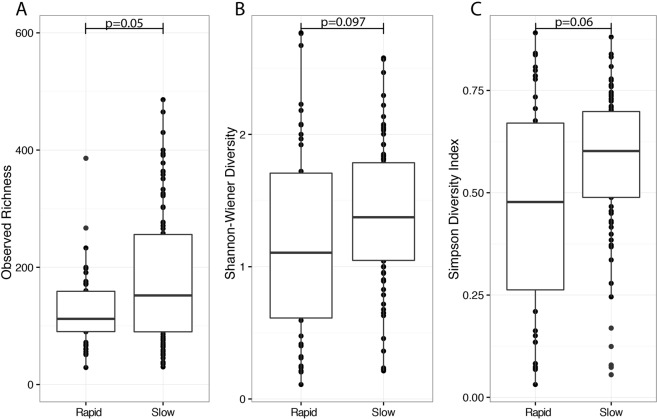
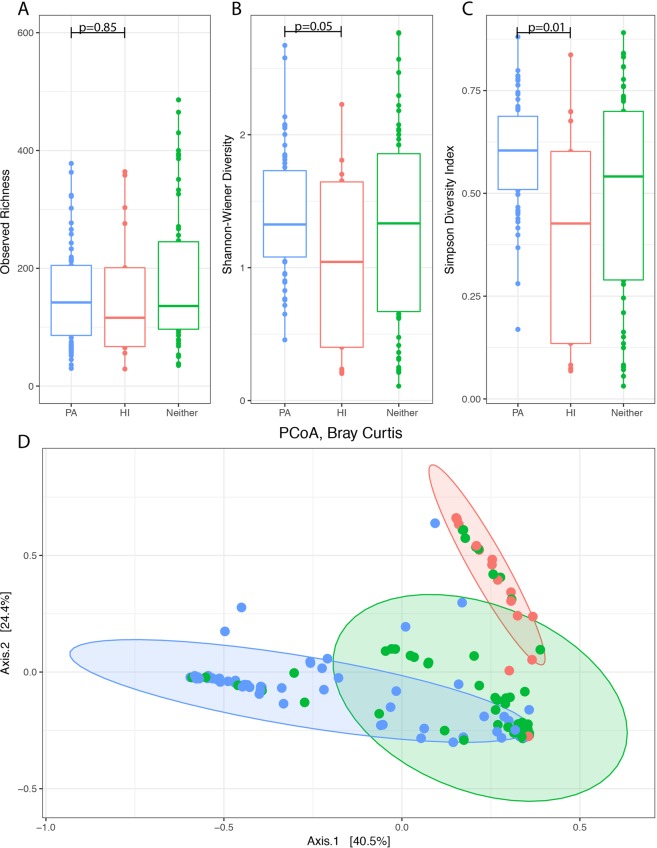
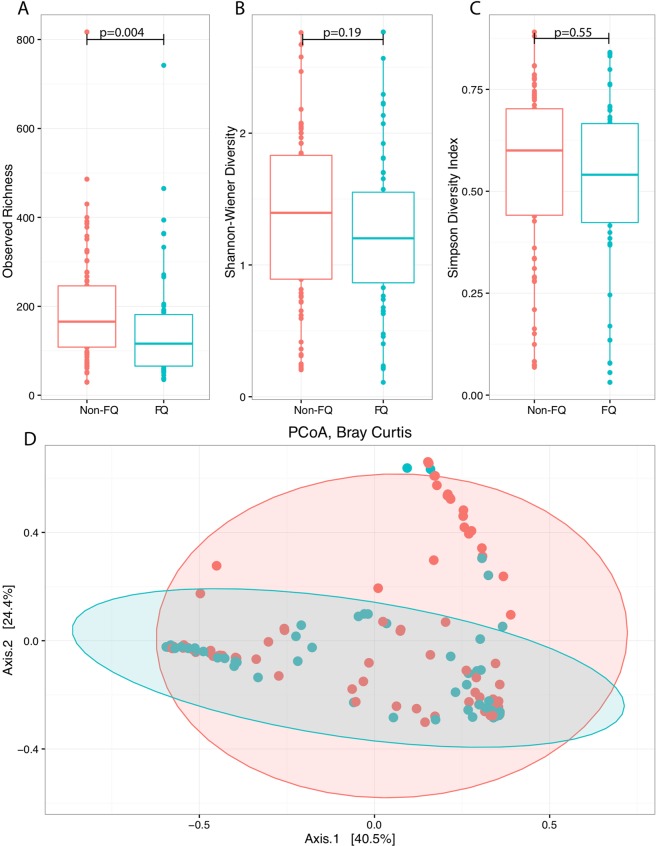
A diverse microbiota exists within the airways of individuals with non-cystic fibrosis bronchiectasis (nCFB). How the lung microbiome evolves over time, and whether changes within the microbiome correlate with future disease progression is not yet known. We assessed the microbial community structure of 133 serial sputa and subsequent disease course of 29 nCFB patients collected over a span of 4-16 years using 16S rRNA paired-end sequencing. Interestingly, no significant shifts in the microbial community of individuals were observed during extended follow-up suggesting the microbiome remains relatively stable over prolonged periods. Samples that were Pseudomonas aeruginosa culture positive displayed markedly different microbial community structures compared to those that were positive for Haemophilus influenzae. Importantly, patients with sputum of lower microbial community diversity were more likely to experience subsequent lung function decline as defined by annual change in ≥-1 FEV1% predicted. Shannon diversity values <1 were more prevalent in patients with FEV1 decline (P = 0.002). However, the relative abundance of particular core microbiota constituents did not associate with risk of decline. Here we present data confirming that the microbiome of nCFB individuals is generally stable, and that microbiome-based measurements may have a prognostic role as biomarkers for nCFB.
Conflict of interest statement
T.E.W., R.L., A.A.H., N.A., C.H.M., R.S. and C.D. declare no competing interests. M.D.P., H.R.R. and M.G.S. have received research support from Gilead Sciences.
Figures
References
-
- Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic Burden of Bronchiectasis. Clin. Pulm. Med. 2005;12:205–209. doi: 10.1097/01.cpm.0000171422.98696.ed. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
