

Compensatory-reserve-weighted intracranial pressure versus intracranial pressure for outcome association in adult traumatic brain injury: a CENTER-TBI validation study
- PMID: 31053909
- PMCID: PMC6581920
- DOI: 10.1007/s00701-019-03915-3
Compensatory-reserve-weighted intracranial pressure versus intracranial pressure for outcome association in adult traumatic brain injury: a CENTER-TBI validation study
Abstract
Background: Compensatory-reserve-weighted intracranial pressure (wICP) has recently been suggested as a supplementary measure of intracranial pressure (ICP) in adult traumatic brain injury (TBI), with a single-center study suggesting an association with mortality at 6 months. No multi-center studies exist to validate this relationship. The goal was to compare wICP to ICP for association with outcome in a multi-center TBI cohort.
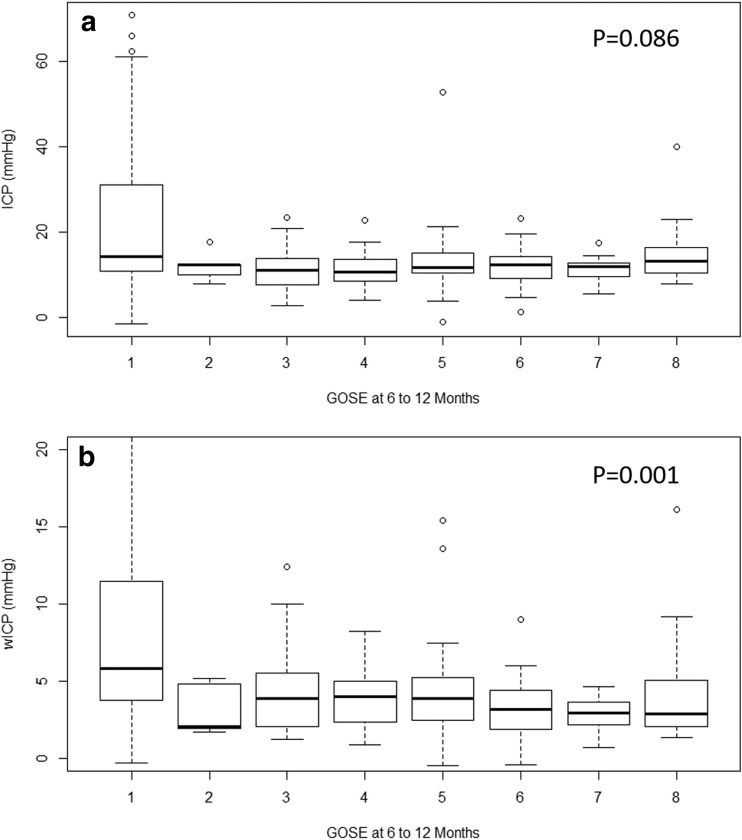
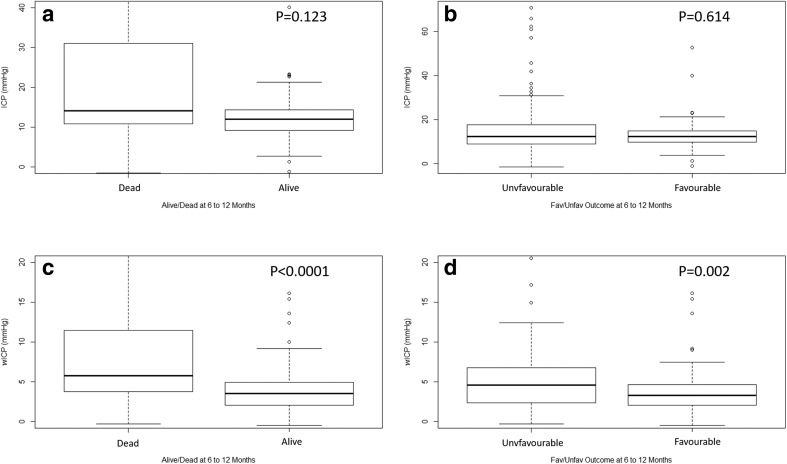
Methods: Using the Collaborative European Neuro Trauma Effectiveness Research in TBI (CENTER-TBI) high-resolution intensive care unit (ICU) cohort, we derived ICP and wICP (calculated as wICP = (1 - RAP) × ICP; where RAP is the compensatory reserve index derived from the moving correlation between pulse amplitude of ICP and ICP). Various univariate logistic regression models were created comparing ICP and wICP to dichotomized outcome at 6 to 12 months, based on Glasgow Outcome Score-Extended (GOSE) (alive/dead-GOSE ≥ 2/GOSE = 1; favorable/unfavorable-GOSE 5 to 8/GOSE 1 to 4, respectively). Models were compared using area under the receiver operating curves (AUC) and p values.
Results: wICP displayed higher AUC compared to ICP on univariate regression for alive/dead outcome compared to mean ICP (AUC 0.712, 95% CI 0.615-0.810, p = 0.0002, and AUC 0.642, 95% CI 0.538-746, p < 0.0001, respectively; no significant difference on Delong's test), and for favorable/unfavorable outcome (AUC 0.627, 95% CI 0.548-0.705, p = 0.015, and AUC 0.495, 95% CI 0.413-0.577, p = 0.059; significantly different using Delong's test p = 0.002), with lower wICP values associated with improved outcomes (p < 0.05 for both). These relationships on univariate analysis held true even when comparing the wICP models with those containing both ICP and RAP integrated area under the curve over time (p < 0.05 for all via Delong's test).
Conclusions: Compensatory-reserve-weighted ICP displays superior outcome association for both alive/dead and favorable/unfavorable dichotomized outcomes in adult TBI, through univariate analysis. Lower wICP is associated with better global outcomes. The results of this study provide multi-center validation of those seen in a previous single-center study.
Keywords: Compensatory reserve; Intracranial pressure; Outcome; Weighted ICP.
Conflict of interest statement
Funding was obtained from the Hannelore Kohl Stiftung (Germany), from OneMind (USA) and from Integra LifeSciences Corporation (USA). PS and MC receive part of licensing fees for the software ICM+ (Cambridge Enterprise Ltd., UK) used for data collection and analysis in this study. All other authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures

References
-
- Adams H, Donnelly J, Czosnyka M, Kolias AG, Helmy A, Menon DK, Smielewski P, Hutchinson PJ. Temporal profile of intracranial pressure and cerebrovascular reactivity in severe traumatic brain injury and association with fatal outcome: an observational study. PLoS Med. 2017;14(7):e1002353. doi: 10.1371/journal.pmed.1002353. - DOI - PMC - PubMed
-
- Calviello L, Donnelly J, Cardim D, Robba C, Zeiler FA, Smielewski P, Czosnyka M (2018) Compensatory-reserve-weighted intracranial pressure and its association with outcome after traumatic brain injury. Neurocrit Care 28(2):212–220. 10.1007/s12028-017-0475-7 - PubMed
-
- Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury, Fourth Edition. Neurosurgery. 2017;80(1):6–15. - PubMed
