

Development and psychometric properties of the "Suicidality: Treatment Occurring in Paediatrics (STOP) Risk and Resilience Factors Scales" in adolescents
- PMID: 31054125
- PMCID: PMC7024696
- DOI: 10.1007/s00787-019-01328-2
Development and psychometric properties of the "Suicidality: Treatment Occurring in Paediatrics (STOP) Risk and Resilience Factors Scales" in adolescents
Abstract
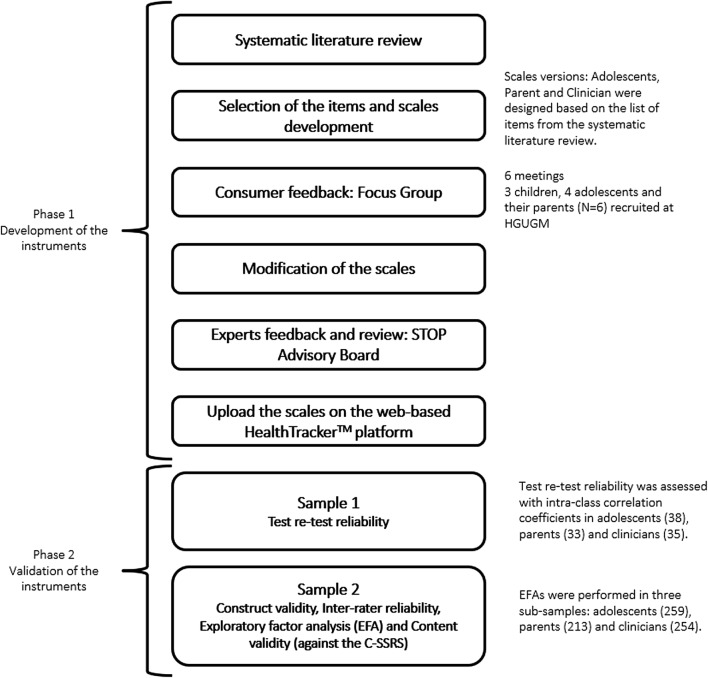
Suicidality in the child and adolescent population is a major public health concern. There is, however, a lack of developmentally sensitive valid and reliable instruments that can capture data on risk, and clinical and psychosocial mediators of suicidality in young people. In this study, we aimed to develop and assess the validity of instruments evaluating the psychosocial risk and protective factors for suicidal behaviours in the adolescent population. In Phase 1, based on a systematic literature review of suicidality, focus groups, and expert panel advice, the risk factors and protective factors (resilience factors) were identified and the adolescent, parent, and clinician versions of the STOP-Suicidality Risk Factors Scale (STOP-SRiFS) and the Resilience Factors Scale (STOP-SReFS) were developed. Phase 2 involved instrument validation and comprised of two samples (Sample 1 and 2). Sample 1 consisted of 87 adolescents, their parents/carers, and clinicians from the various participating centres, and Sample 2 consisted of three sub-samples: adolescents (n = 259) who completed STOP-SRiFS and/or the STOP-SReFS scales, parents (n = 213) who completed one or both of the scales, and the clinicians who completed the scales (n = 254). The STOP-SRiFS demonstrated a good construct validity-the Cronbach Alpha for the adolescent (α = 0.864), parent (α = 0.842), and clinician (α = 0.722) versions of the scale. Test-retest reliability, inter-rater reliability, and content validity were good for all three versions of the STOP-SRiFS. The sub-scales generated using Exploratory Factor Analysis (EFA) were the (1) anxiety and depression risk, (2) substance misuse risk, (3) interpersonal risk, (4) chronic risk, and (5) risk due to life events. For the STOP-SRiFS, statistically significant correlations were found between the Columbia-Suicide Severity Rating Scale (C-SSRS) total score and the adolescent, parent, and clinical versions of the STOP-SRiFS sub-scale scores. The STOP-SRiFS showed good psychometric properties. This study demonstrated a good construct validity for the STOP-SReFS-the Cronbach Alpha for the three versions were good (adolescent: α = 0.775; parent: α = 0.808; α = clinician: 0.808). EFA for the adolescent version of the STOP-SReFS, which consists of 9 resilience factors domains, generated two factors (1) interpersonal resilience and (2) cognitive resilience. The STOP-SReFS Cognitive Resilience sub-scale for the adolescent was negatively correlated (r = - 0.275) with the C-SSRS total score, showing that there was lower suicidality in those with greater Cognitive Resilience. The STOP-SReFS Interpersonal resilience sub-scale correlations were all negative, but none of them were significantly different to the C-SSRS total scores for either the adolescent, parent, or clinician versions of the scales. This is not surprising, because the items in this sub-scale capture a much larger time-scale, compared to the C-SSRS rating period. The STOP-SReFS showed good psychometric properties. The STOP-SRiFS and STOP-SReFS are instruments that can be used in future studies about suicidality in children and adolescents.
Keywords: Adolescents; Children; Psychosocial; Questionnaire development and validation; Resilience; Risk; Suicidality.
Conflict of interest statement
Professor Paramala Santosh is Director & CEO and stockholder in HealthTracker Ltd. Dr. F. Fiori is Chief Technology Officer employed by HealthTracker Ltd. Dr. K. Lievesley is a Programme Manager employed at HealthTracker Ltd. Dr. Rodríguez-Quiroga has previously held a Río Hortega grant, Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness. Dr. Díaz-Caneja has previously held a Río Hortega grant, Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness, and a Grant from Fundación Alicia Koplowitz. Dr. Dittmann has received compensation for serving as consultant or speaker, or he or the institution he works for have received research support or royalties from the organizations or companies indicated: EU (FP7 Programme), US National Institute of Mental Health (NIMH), German Federal Ministry of Health/Regulatory Agency (BMG/BfArM), German Federal Ministry of Education and Research (BMBF), German Research Foundation (DFG), Volkswagen Foundation; Boehringer Ingelheim, Ferring, Janssen-Cilag, Lilly, Lundbeck, Otsuka, Servier, Shire, Sunovion/Takeda, and Theravance. Dr. Dittmann owns Eli Lilly stock. Dr. Zuddas has been a consultant to or has received honoraria or grants from EU (FP7 Programme), Angelini, Lundbeck, Janssen, Roche, Servier, Shire, Takeda, and Vifor. Prof. Coghill reports grants and personal fees from Shire, personal fees from Janssen-Cilag, personal fees from Lilly, grants and personal fees from Vifor, personal fees from Novartis, personal fees from Flynn Pharma, personal fees from Medice, and personal fees from Oxford University Press, outside the submitted work. Dr. Arango has been a consultant to or has received honoraria or grants from Acadia, Abbot, AMGEN, AstraZeneca, Bristol-Myers Squibb, Janssen-Cilag, Lundbeck, Merck, Otsuka, Pfizer, Roche, Servier, Sumitomo-Dainippon Pharma, Shire, Takeda, Teva, and Schering Plough. Dr Purper-Ouakil has been consultant for Shire, Boiron, and Mensia, and has received honoraria or travel grants from Shire, Otsuka, Medice, Jannssen-Cilag, and Ardix. None of the other authors have any conflicts of interest or disclosures to declare. Part of these data have been included in an FP7 STOP Report to the European Union.
Figures
References
-
- World Health Organization (1989) World report on violence and health, P 2002
