

Detection of familial hypercholesterolaemia: external validation of the FAMCAT clinical case-finding algorithm to identify patients in primary care
- PMID: 31054643
- PMCID: PMC6506568
- DOI: 10.1016/S2468-2667(19)30061-1
Detection of familial hypercholesterolaemia: external validation of the FAMCAT clinical case-finding algorithm to identify patients in primary care
Erratum in
-
Correction to Lancet Public Health 2019; 4: e256-64.Lancet Public Health. 2019 Jul;4(7):e325. doi: 10.1016/S2468-2667(19)30113-6. Lancet Public Health. 2019. PMID: 31279416 Free PMC article. No abstract available.
Abstract
Background: The vast majority of individuals with familial hypercholesterolaemia in the general population remain unidentified worldwide. Recognising patients most likely to have the condition, to enable targeted specialist assessment and treatment, could prevent major coronary morbidity and mortality. We aimed to evaluate a clinical case-finding algorithm, the familial hypercholesterolaemia case ascertainment tool (FAMCAT), and compare it with currently recommended methods for detection of familial hypercholesterolaemia in primary care.
Methods: In this external validation study, FAMCAT regression equations were applied to a retrospective cohort of patients aged 16 years or older with cholesterol assessed, who were randomly selected from 1500 primary care practices across the UK contributing to the QResearch database. In the main analysis, we assessed the ability of FAMCAT to detect familial hypercholesterolaemia (ie, its discrimination) and compared it with that of other established clinical case-finding approaches recommended internationally (Simon Broome, Dutch Lipid Clinic Network, Make Early Diagnosis to Prevent Early Deaths [MEDPED] and cholesterol concentrations higher than the 99th percentile of the general population in the UK). We assessed discrimination by area under the receiver operating curve (AUROC; ranging from 0·5, indicating pure chance, to 1, indicating perfect discrimination). Using a probability threshold of more than 1 in 500 (prevalence of familial hypercholesterolaemia), we also assessed sensitivity, specificity, positive predictive values, and negative predictive values in the main analysis.
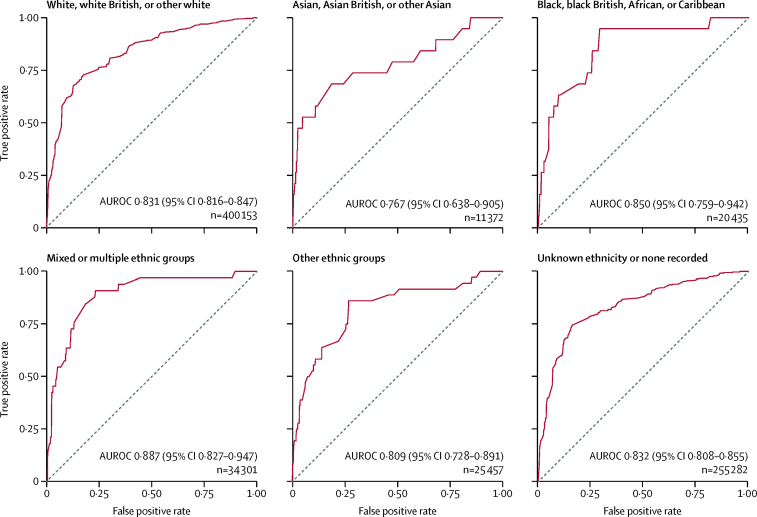
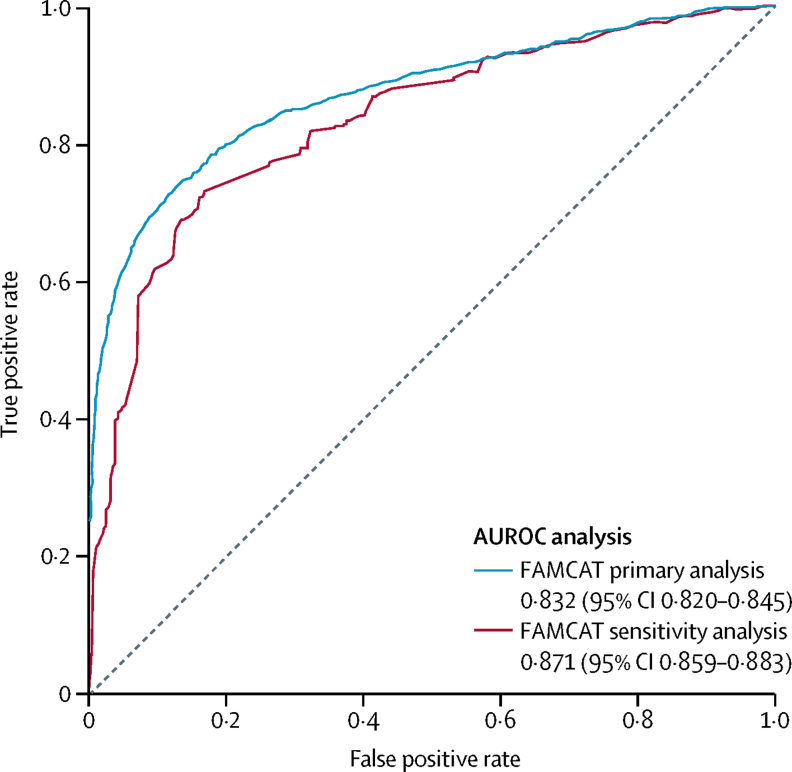
Findings: A sample of 750 000 patients who registered in 1500 UK primary care practices that contribute anonymised data to the QResearch database between Jan 1, 1999, and Sept 1, 2017, was randomly selected, of which 747 000 patients were assessed. FAMCAT showed a high degree of discrimination (AUROC 0·832, 95% CI 0·820-0·845), which was higher than that of Simon Broome criteria (0·694, 0·681-0·703), Dutch Lipid Clinic Network criteria (0·724, 0·710-0·738), MEDPED criteria (0·624, 0·609-0·638), and screening cholesterol concentrations higher than the 99th percentile (0·581, 0·570-0·591). Using a 1 in 500 probability threshold, FAMCAT achieved a sensitivity of 84% (1028 predicted vs 1219 observed cases) and specificity of 60% (443 949 predicted vs 745 781 observed non-cases), with a corresponding positive predictive value of 0·84% and a negative predictive value of 99·2%.
Interpretation: FAMCAT identifies familial hypercholesterolaemia with greater accuracy than currently recommended approaches and could be considered for clinical case finding of patients with the highest likelihood of having hypercholesterolaemia in primary care.
Funding: UK National Institute for Health Research School for Primary Care Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
A window into the heart of familial hypercholesterolaemia in the community.Lancet Public Health. 2019 May;4(5):e216-e217. doi: 10.1016/S2468-2667(19)30055-6. Lancet Public Health. 2019. PMID: 31054637 No abstract available.
References
-
- Austin MA, Hutter CM, Zimmern RL, Humphries SE. Genetic causes of monogenic heterozygous familial hypercholesterolemia: a HuGE prevalence review. Am J Epidemiol. 2004;160:407–420. - PubMed
-
- Marks D, Thorogood M, Neil HA, Humphries SE. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis. 2003;168:1–14. - PubMed
-
- Nordestgaard BG, Chapman MJ, Humphries SE. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34:3478. 390a. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
