

Door-to-Targeted Temperature Management Initiation Time and Outcomes in Out-of-Hospital Cardiac Arrest: Insights From the Continuous Chest Compressions Trial
- PMID: 31055981
- PMCID: PMC6512141
- DOI: 10.1161/JAHA.119.012001
Door-to-Targeted Temperature Management Initiation Time and Outcomes in Out-of-Hospital Cardiac Arrest: Insights From the Continuous Chest Compressions Trial
Abstract
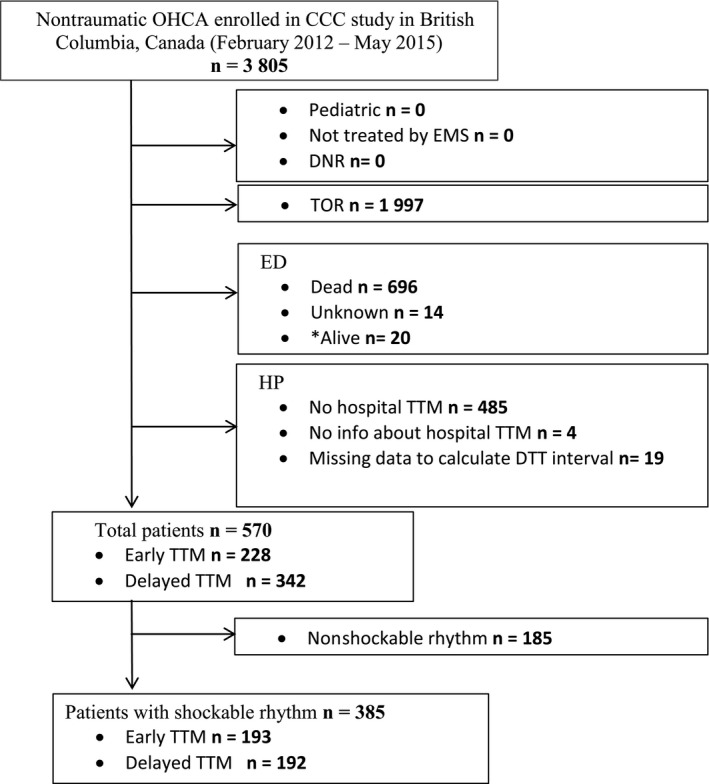
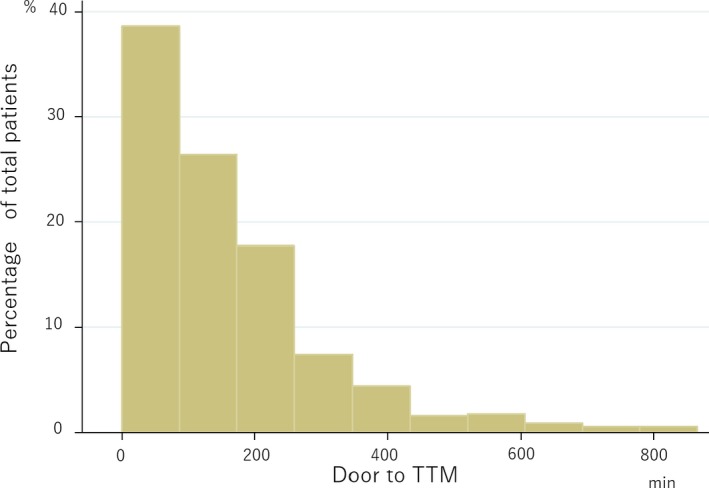
Background Targeted temperature management ( TTM ) is a recommended treatment modality to improve neurological outcomes in patients with out-of-hospital cardiac arrest. The impact of the duration from hospital admission to TTM initiation (door-to- TTM ; DTT ) on clinical outcomes has not been well elucidated. We hypothesized that shorter DTT initiation intervals would be associated with improved survival with favorable neurological outcome. Methods and Results We performed a post hoc analysis of nontraumatic paramedic-treated out-of-hospital cardiac arrests. The primary outcome was favorable neurological status at hospital discharge, with a secondary outcome of survival to discharge. We fit a logistic regression analysis to determine the association of early compared with delayed DTT , dichotomized by the median DTT duration, and outcomes. Of 3805 patients enrolled in the CCC (Continuous Chest Compressions) Trial in British Columbia, 570 were included in this analysis. There was substantial variation in DTT among patients receiving TTM . The median DTT duration was 122 minutes (interquartile range 35-218). Favorable neurological outcomes in the early and delayed DTT groups were 48% and 38%, respectively. Compared with delayed DTT (interquartile range 167-319 minutes), early DTT (interquartile range 20-81 minutes) was associated with survival (adjusted odds ratio 1.56, 95% CI 1.02-2.38) but not with favorable neurological outcomes (adjusted odds ratio 1.45, 95% CI , 0.94-2.22) at hospital discharge. Conclusions There was wide variability in the initiation of TTM among comatose out-of-hospital cardiac arrest survivors. Initiation of TTM within 122 minutes of hospital admission was associated with improved survival. These results support in-hospital efforts to achieve early DTT among out-of-hospital cardiac arrest patients admitted to the hospital.
Keywords: cardiac arrest; cardiac arrhythmia; neurocritical care; neuroprotectant; survival.
Figures
Comment in
-
Door-to-Targeted Temperature Management Initiation After Out-of-Hospital Cardiac Arrest: A New Quality Metric in Postresuscitation Care?J Am Heart Assoc. 2019 May 7;8(9):e012666. doi: 10.1161/JAHA.119.012666. J Am Heart Assoc. 2019. PMID: 31057012 Free PMC article.
References
-
- Uribarri A, Bueno H, Pérez‐Castellanos A, Loughlin G, Sousa I, Viana‐Tejedor A, Fernandez‐Aviles F. Impact of time to cooling initiation and time to target temperature in patients treated with hypothermia after cardiac arrest. Eur Heart J Acute Cardiovasc Care. 2015;4:365–372. - PubMed
-
- Grunau B, Kawano T, Dick W, Straight R, Connolly H, Schlamp R, Scheuermeyer F, Fordyce CF, Barbic D, Tallon J, Christenson J. Trends in care processes and survival following prehospital resuscitation improvement initiatives for out‐of‐hospital cardiac arrest in British Columbia, 2006–2012. Resuscitation. 2018;125:118–125. - PubMed
-
- Hypothermia After Cardiac Arrest Study Group . Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutterridge G, Smith K. Treatment of comatose survivors of out‐of‐hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
