

Cellular Immune Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
- PMID: 31057538
- PMCID: PMC6477089
- DOI: 10.3389/fimmu.2019.00796
Cellular Immune Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
Abstract
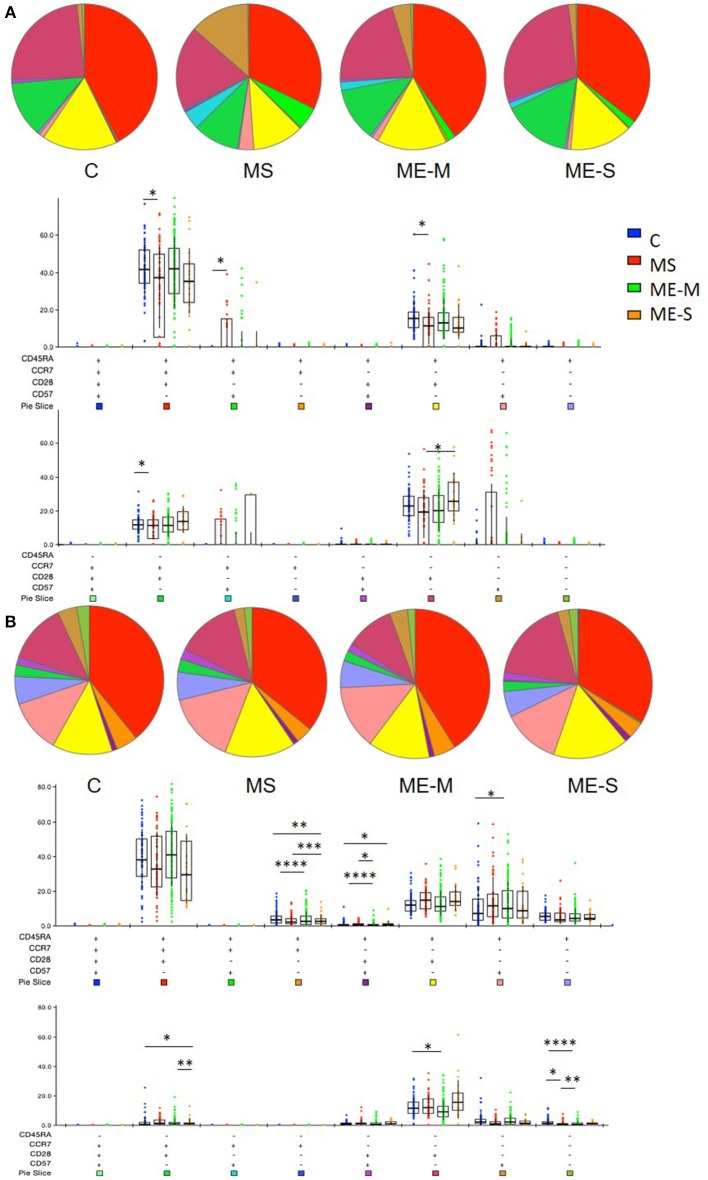
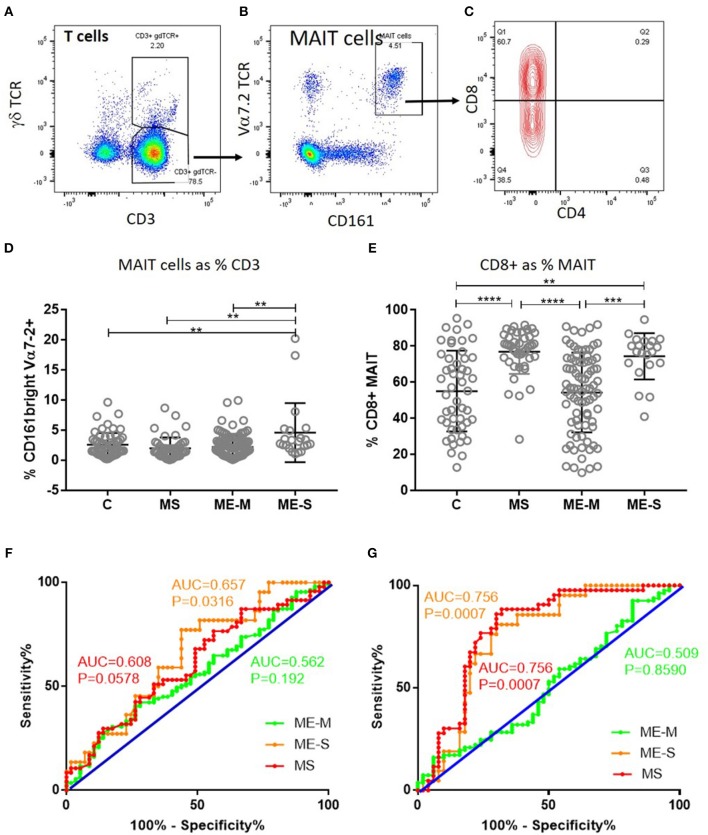
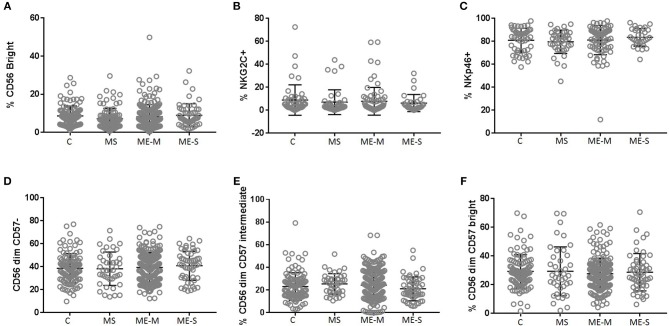
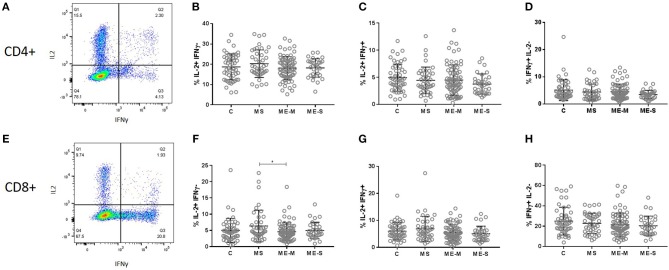
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a debilitating condition with unknown aetiology, Myalgic encephalomyelitis unclear pathophysiology and with no diagnostic test or biomarker available. Many patients report their ME/CFS began after an acute infection, and subsequent increased frequency of infections, such as colds or influenza, is common. These factors imply an altered immunological status exists in ME/CFS, in at least a proportion of patients, yet previous studies of peripheral immunity have been discrepant and inconclusive. The UK ME/CFS Biobank, which has collected blood samples from nearly 300 clinically-confirmed ME/CFS patients, enables large-scale studies of immunological function in phenotypically well-characterised participants. In this study, herpes virus serological status and T cell, B cell, NK cell and monocyte populations were investigated in 251 ME/CFS patients, including 54 who were severely affected, and compared with those from 107 healthy participants and with 46 patients with Multiple Sclerosis. There were no differences in seroprevalence for six human herpes viruses between ME/CFS and healthy controls, although seroprevalence for the Epstein-Barr virus was higher in multiple sclerosis patients. Contrary to previous reports, no significant differences were observed in NK cell numbers, subtype proportions or in vitro responsiveness between ME/CFS patients and healthy control participants. In contrast, the T cell compartment was altered in ME/CFS, with increased proportions of effector memory CD8+ T cells and decreased proportions of terminally differentiated effector CD8+ T cells. Conversely, there was a significantly increased proportion of mucosal associated invariant T cells (MAIT) cells, especially in severely affected ME/CFS patients. These abnormalities demonstrate that an altered immunological state does exist in ME/CFS, particularly in severely affected people. This may simply reflect ongoing or recent infection, or may indicate future increased susceptibility to infection. Longitudinal studies of ME/CFS patients are needed to help to determine cause and effect and thus any potential benefits of immuno-modulatory treatments for ME/CFS.
Keywords: MAIT cells; T cell differentiation; chronic fatigue syndrome; herpes viruses; myalgic encephalomyelitis; natural killer cells.
Figures
Similar articles
-
Surveying the Metabolic and Dysfunctional Profiles of T Cells and NK Cells in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.Int J Mol Sci. 2023 Jul 26;24(15):11937. doi: 10.3390/ijms241511937. Int J Mol Sci. 2023. PMID: 37569313 Free PMC article. Review.
-
Cytomegalovirus, Epstein-Barr virus, and human herpesvirus-6 infections in patients with myalgic еncephalomyelitis/chronic fatigue syndrome.J Med Virol. 2020 Dec;92(12):3682-3688. doi: 10.1002/jmv.25744. Epub 2020 Mar 11. J Med Virol. 2020. PMID: 32129496 Free PMC article.
-
Characterisation of cell functions and receptors in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME).BMC Immunol. 2015 Jun 2;16:35. doi: 10.1186/s12865-015-0101-4. BMC Immunol. 2015. PMID: 26032326 Free PMC article.
-
Antibodies to Human Herpesviruses in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients.Front Immunol. 2019 Aug 14;10:1946. doi: 10.3389/fimmu.2019.01946. eCollection 2019. Front Immunol. 2019. PMID: 31475007 Free PMC article.
-
Epstein-Barr Virus and the Origin of Myalgic Encephalomyelitis or Chronic Fatigue Syndrome.Front Immunol. 2021 Nov 15;12:656797. doi: 10.3389/fimmu.2021.656797. eCollection 2021. Front Immunol. 2021. PMID: 34867935 Free PMC article. Review.
Cited by
-
Biomarkers for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a systematic review.BMC Med. 2023 May 24;21(1):189. doi: 10.1186/s12916-023-02893-9. BMC Med. 2023. PMID: 37226227 Free PMC article.
-
Health Care Responsibility and Compassion-Visiting the Housebound Patient Severely Affected by ME/CFS.Healthcare (Basel). 2020 Jul 4;8(3):197. doi: 10.3390/healthcare8030197. Healthcare (Basel). 2020. PMID: 32635535 Free PMC article.
-
Altered endothelial dysfunction-related miRs in plasma from ME/CFS patients.Sci Rep. 2021 May 19;11(1):10604. doi: 10.1038/s41598-021-89834-9. Sci Rep. 2021. PMID: 34011981 Free PMC article.
-
Surveying the Metabolic and Dysfunctional Profiles of T Cells and NK Cells in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.Int J Mol Sci. 2023 Jul 26;24(15):11937. doi: 10.3390/ijms241511937. Int J Mol Sci. 2023. PMID: 37569313 Free PMC article. Review.
-
The Neurological Manifestations of Post-Acute Sequelae of SARS-CoV-2 infection.Curr Neurol Neurosci Rep. 2021 Jun 28;21(9):44. doi: 10.1007/s11910-021-01130-1. Curr Neurol Neurosci Rep. 2021. PMID: 34181102 Free PMC article. Review.
References
-
- Carruthers B, Jain AK, De Meirleir KL, Peterson DL, Klimas NG, Lerner AM, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: clinical working case definition, diagnostic and treatment guidelines a consensus document. J Chronic Fat Syndr. (2003) 11:7–115. 10.1300/J092v11n01_02 - DOI
-
- Kingdon CC, Bowman EW, Curran H, Nacul L, Lacerda EM. Functional status and well-being in people with myalgic encephalomyelitis/chronic fatigue syndrome compared with people with multiple sclerosis and healthy controls. Pharmacoecon Open. (2018) 2:381–92. 10.1007/s41669-018-0071-6 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials