

Refractory Vasospastic Angina: When Typical Medications Don't Work
- PMID: 31058017
- PMCID: PMC6485519
- DOI: 10.7759/cureus.4134
Refractory Vasospastic Angina: When Typical Medications Don't Work
Abstract
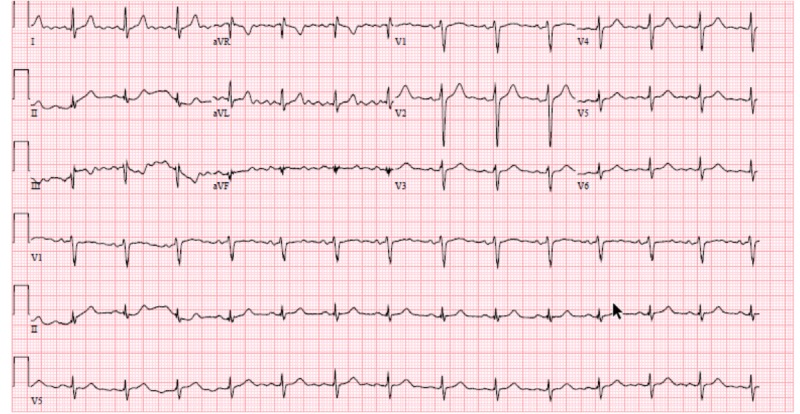
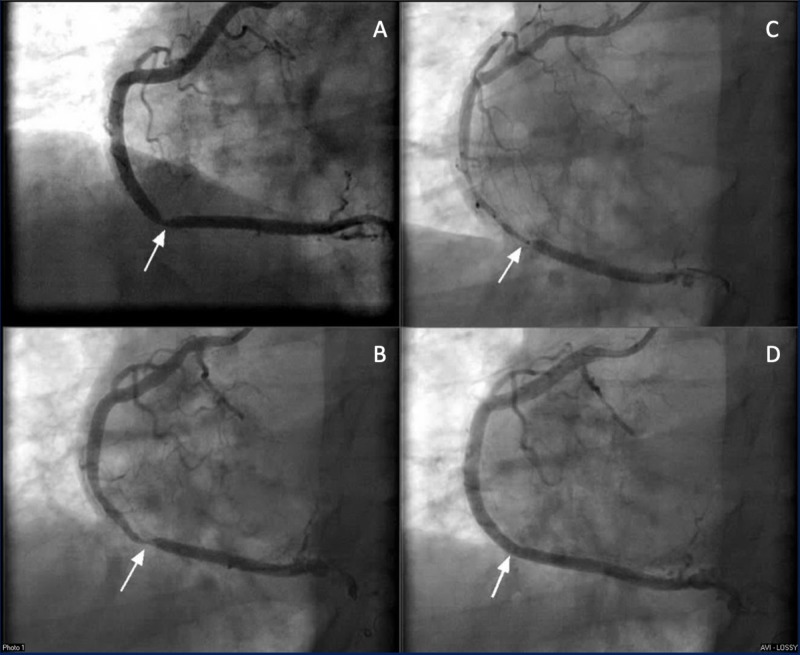
Vasospastic angina (VSA) is defined as spasm of the coronaries leading to transient constriction and eventual myocardial ischemia. VSA is treated typically with calcium-channel blockers (CCBs) and nitrates. However, there are times when the vasospasm is refractory to typical medications. When this occurs, unconventional treatment modalities may be employed for symptomatic relief. We present a case of a 48-year-old-male with a history of inferior ST-elevation myocardial infarction (STEMI) status post percutaneous coronary intervention (PCI) with drug-eluting stent (DES) to the distal right coronary artery (RCA), who presented with recurrent angina. The pain was described as pressure-like, substernal, radiating to both arms, and similar to his previous STEMI presentation. On presentation to the emergency room, he had an elevated serum troponin with no electrocardiogram (EKG) changes. He was taken to the cath lab where it was found that he revealed severe focal stenosis just proximal to the previously placed stent. Immediately after guidewire passage into the RCA, acute vasospasm developed, resulting in diffuse, severe stenosis, extending over previously normal segments to the proximal RCA, resolving with intracoronary nicardipine and nitroglycerin, including the initial focal stenosis. The patient was diagnosed with VSA. Unfortunately, despite optimal medical therapy, he developed refractory VSA, requiring the use of unconventional treatment methods. Our patient presented with a lesser-known phenomenon called refractory VSA, where intermittent vasospasm continues despite being on a combination of two medications. Treatment for VSA is well-documented, however, little data is available for refractory VSA.
Keywords: acute coronary syndrome; nstemi; prinzmetal angina; refractory vasospastic angina; stemi; vasospastic angina.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Some account of a disorder of the breast. Heberden W. Medical Transactions of the Royal College of Physicians. 1772;2:59–67.
-
- Angina pectoris I. A variant form of angina pectoris. Prinzmetal M, Kennamer R, Merliss R, Wada T, Bor N. Am J Med. 1959;27:375–388. - PubMed
-
- The who, what, why, when, how and where of vasospastic angina. Beltrame JF, Crea F, Kaski JC, et al. https://www.ncbi.nlm.nih.gov/pubmed/26686994. Circ J. 2015;80:289–298. - PubMed
-
- Pharmacotherapy of vasospastic angina. Harris JR, Hale GM, Dasari TW, Schwier NC. J Cardiovasc Pharmacol Ther. 2016;21:439–451. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous