

Neonatal Encephalopathy: Need for Recognition of Multiple Etiologies for Optimal Management
- PMID: 31058120
- PMCID: PMC6477286
- DOI: 10.3389/fped.2019.00142
Neonatal Encephalopathy: Need for Recognition of Multiple Etiologies for Optimal Management
Abstract
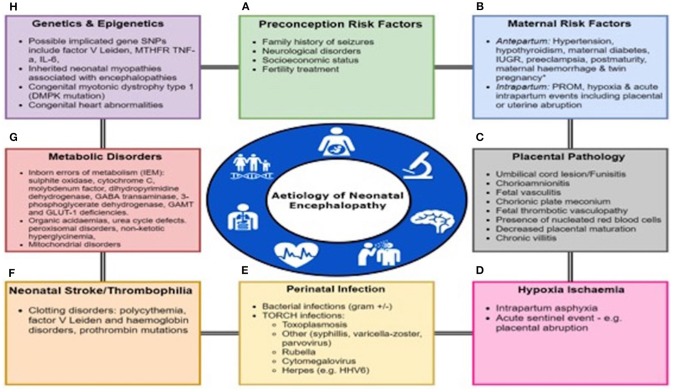
Neonatal encephalopathy (NE) is associated with high mortality and morbidity. Factors predisposing to NE can be antenatal, perinatal, or a combination of both. Antenatal maternal factors, familial factors, genetic predisposition, hypoxic ischemic encephalopathy, infections, placental abnormalities, thrombophilia, coagulation defects, and metabolic disorders all have been implicated in the pathogenesis of NE. At present, therapeutic hypothermia is the only treatment available, regardless of etiology. Recognizing the etiology of NE involved can also guide investigations such as metabolic and sepsis workups to ensure optimal management. Understanding the etiology of NE may allow the development of targeted adjunctive therapies related to the underlying mechanism and develop preventative strategies.
Keywords: antenatal; etiology; neonatal encephalopthy; perinatal; targeted adjunctive therapies.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources