

Clinical Valve Thrombosis and Subclinical Leaflet Thrombosis Following Transcatheter Aortic Valve Replacement: Is There a Need for a Patient-Tailored Antithrombotic Therapy?
- PMID: 31058168
- PMCID: PMC6482296
- DOI: 10.3389/fcvm.2019.00044
Clinical Valve Thrombosis and Subclinical Leaflet Thrombosis Following Transcatheter Aortic Valve Replacement: Is There a Need for a Patient-Tailored Antithrombotic Therapy?
Abstract
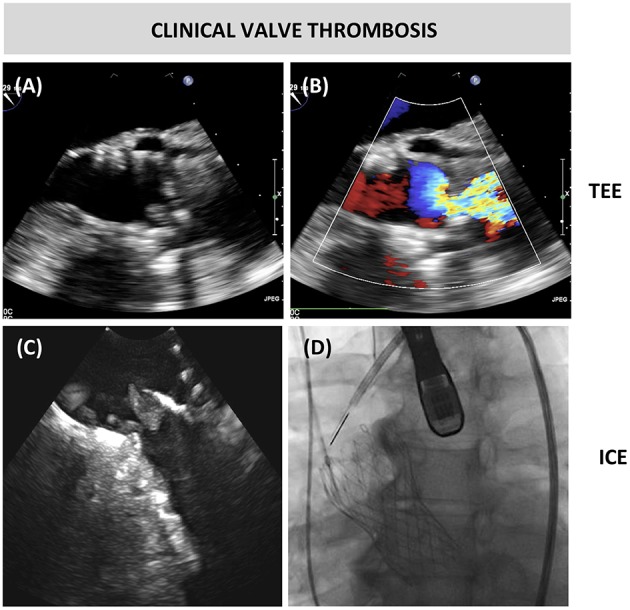
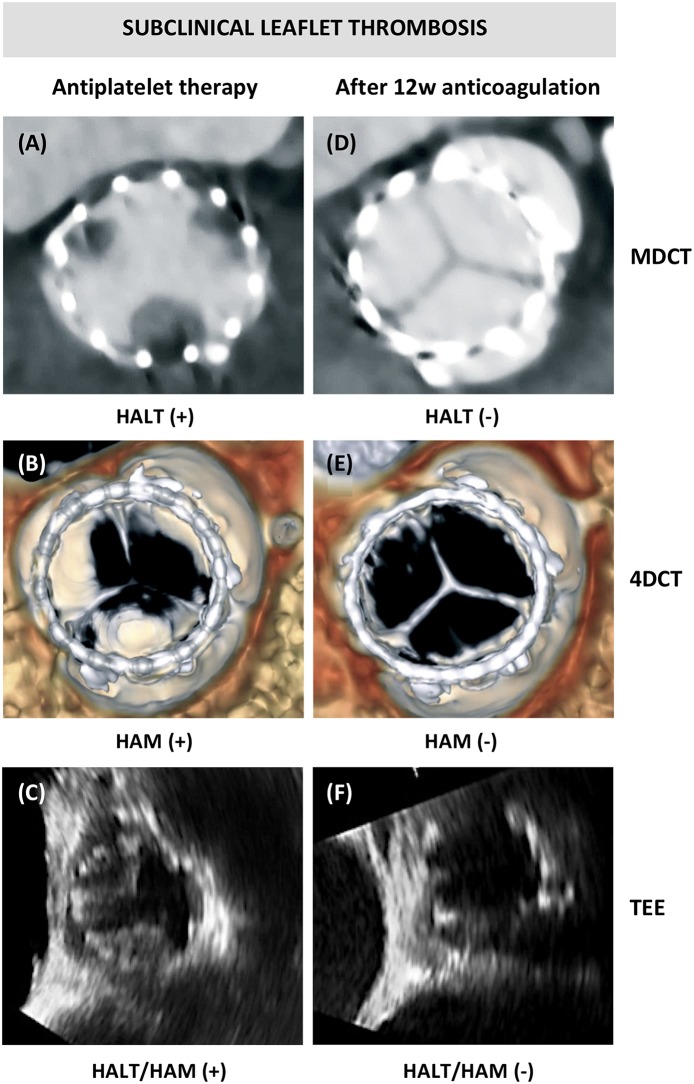
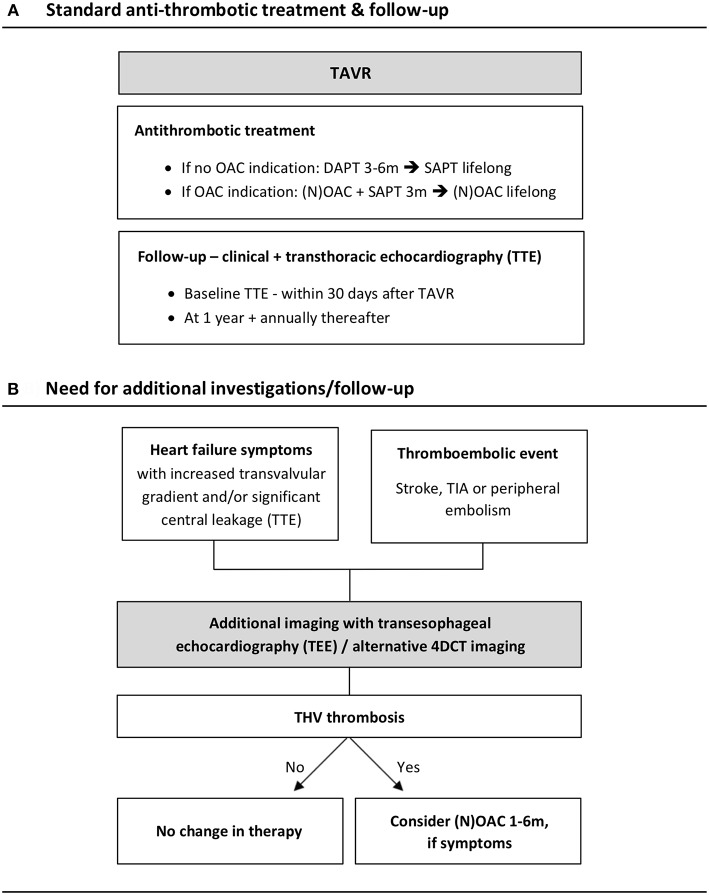
Transcatheter aortic valve replacement (TAVR) has become an established therapeutic option for patients with symptomatic, severe aortic valve stenosis at increased surgical risk. Antithrombotic therapy after TAVR aims to prevent transcatheter heart valve (THV) thrombosis, in which two different entities have to be recognized: clinical valve thrombosis and subclinical leaflet thrombosis. In clinical valve thrombosis, obstructive thrombus formation leads to an increased transvalvular gradient, often provoking heart failure symptoms. Subclinical leaflet thrombosis is most often an incidental finding, characterized by a thin layer of thrombus covering the aortic side of one or more leaflets; it is also referred to as Hypo-Attenuating Leaflet Thickening (HALT) as described on multi-detector computed tomography (MDCT) imaging. This phenomenon may also affect leaflet motion and is then classified as Hypo-Attenuation affecting Motion (HAM). Even in case of HAM, the transvalvular pressure gradient remains within normal range and does not provoke heart failure symptoms. Whereas, clinical valve thrombosis requires treatment, the clinical impact and need for intervention in subclinical leaflet thrombosis is still uncertain. Oral anticoagulant therapy protects against and resolves both clinical valve thrombosis and subclinical leaflet thrombosis; however, large-scale randomized clinical trials studying different antithrombotic strategies after TAVR are still under way. This review article summarizes the currently available data within the field of transcatheter aortic valve/leaflet thrombosis and discusses the need for a patient tailored antithrombotic approach.
Keywords: antithrombotic therapy; aortic valve replacement; clinical valve thrombosis; subclinical leaflet thrombosis; transcatheter.
Figures
References
-
- Søndergaard L, Steinbrüchel DA, Ihlemann N, Nissen H, Kieldsen BJ, Petursson P, et al. . Two-year outcomes in patients with severe aortic valve stenosis randomized to transcatheter versus surgical aortic valve replacement: the all-comers Nordic aortic valve intervention randomized clinical trial. Circ Cardiovasc Interv. (2016) 9:e003665. 10.1161/CIRCINTERVENTIONS.115.003665 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources