

An Organizational-Level Program of Intervention for AKI: A Pragmatic Stepped Wedge Cluster Randomized Trial
- PMID: 31058607
- PMCID: PMC6405151
- DOI: 10.1681/ASN.2018090886
An Organizational-Level Program of Intervention for AKI: A Pragmatic Stepped Wedge Cluster Randomized Trial
Abstract
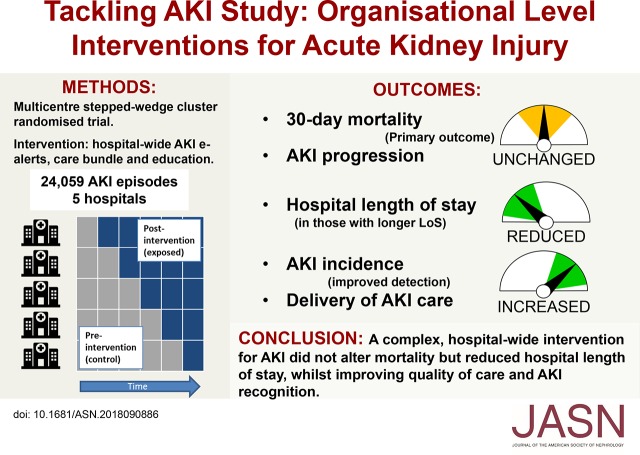
Background: Variable standards of care may contribute to poor outcomes associated with AKI. We evaluated whether a multifaceted intervention (AKI e-alerts, an AKI care bundle, and an education program) would improve delivery of care and patient outcomes at an organizational level.
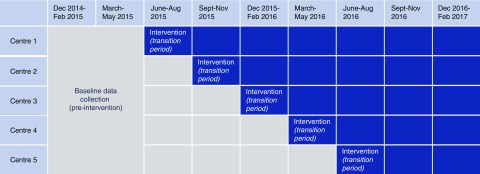
Methods: A multicenter, pragmatic, stepped-wedge cluster randomized trial was performed in five UK hospitals, involving patients with AKI aged ≥18 years. The intervention was introduced sequentially across fixed three-month periods according to a randomly determined schedule until all hospitals were exposed. The primary outcome was 30-day mortality, with pre-specified secondary endpoints and a nested evaluation of care process delivery. The nature of the intervention precluded blinding, but data collection and analysis were independent of project delivery teams.
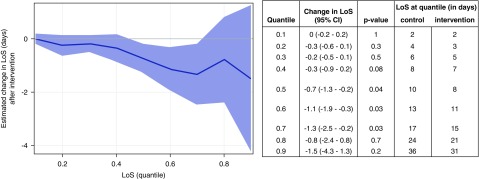
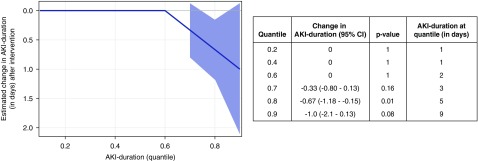
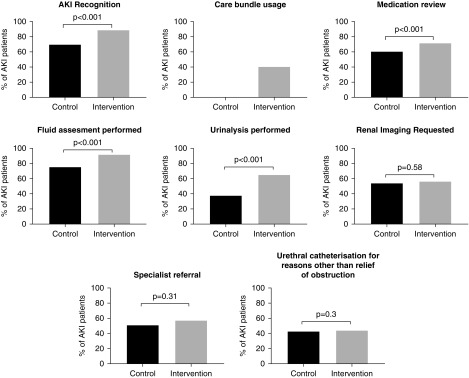
Results: We studied 24,059 AKI episodes, finding an overall 30-day mortality of 24.5%, with no difference between control and intervention periods. Hospital length of stay was reduced with the intervention (decreases of 0.7, 1.1, and 1.3 days at the 0.5, 0.6, and 0.7 quantiles, respectively). AKI incidence increased and was mirrored by an increase in the proportion of patients with a coded diagnosis of AKI. Our assessment of process measures in 1048 patients showed improvements in several metrics including AKI recognition, medication optimization, and fluid assessment.
Conclusions: A complex, hospital-wide intervention to reduce harm associated with AKI did not reduce 30-day AKI mortality but did result in reductions in hospital length of stay, accompanied by improvements in in quality of care. An increase in AKI incidence likely reflected improved recognition.
Keywords: AKI; acute renal failure; care bundle; clinical nephrology; e-alert; education.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
A Pragmatic Step Forward: AKI and Beyond.J Am Soc Nephrol. 2019 Mar;30(3):371-372. doi: 10.1681/ASN.2019010076. Epub 2019 Feb 21. J Am Soc Nephrol. 2019. PMID: 31062701 Free PMC article. No abstract available.
References
-
- Lameire NH, Bagga A, Cruz D, De Maeseneer J, Endre Z, Kellum JA, et al.: Acute kidney injury: An increasing global concern. Lancet 382: 170–179, 2013 - PubMed
-
- Vanmassenhove J, Kielstein J, Jörres A, Biesen WV: Management of patients at risk of acute kidney injury. Lancet 389: 2139–2151, 2017 - PubMed
-
- KDIGO AKI Work Group : Clinical practice guideline for acute kidney injury. Kidney Int Suppl 2[Suppl 1]: 1–141, 2012
-
- Lewington A, Kanagasundaram S: Renal association clinical practice guidelines on acute kidney injury. Nephron Clin Pract 118[Suppl 1]: c349–c390, 2011 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
