

The Association of Fever and Antipyretic Medication With Outcomes in Mechanically Ventilated Patients: A Cohort Study
- PMID: 31058720
- PMCID: PMC6629479
- DOI: 10.1097/SHK.0000000000001368
The Association of Fever and Antipyretic Medication With Outcomes in Mechanically Ventilated Patients: A Cohort Study
Abstract
Background: Fever is common in mechanically ventilated patients and may be uniquely detrimental in those with lung injury because of its injurious effects on pulmonary vascular permeability and alveolar epithelium. We evaluated the association of fever and antipyretic medication with mortality in mechanically ventilated emergency department (ED) patients.
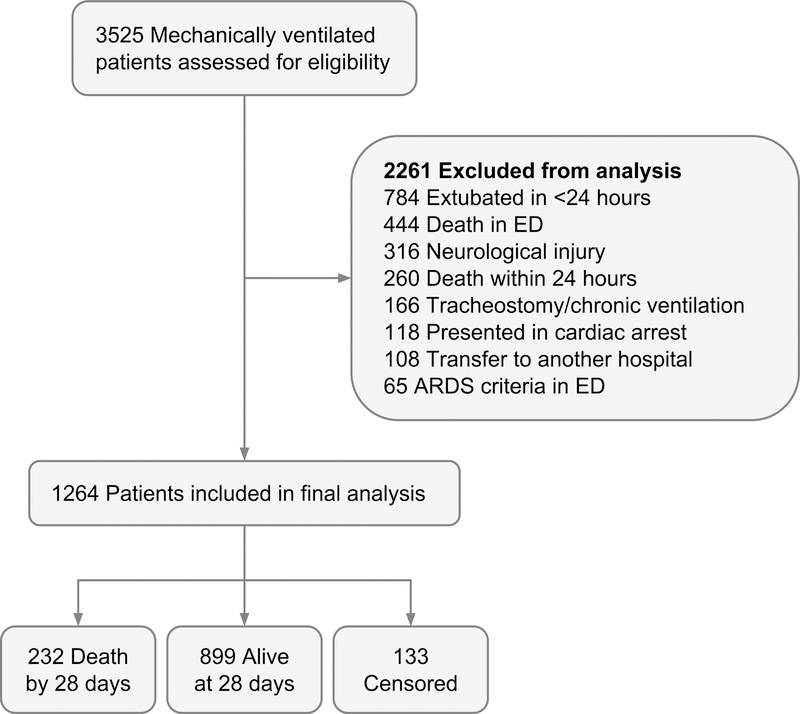
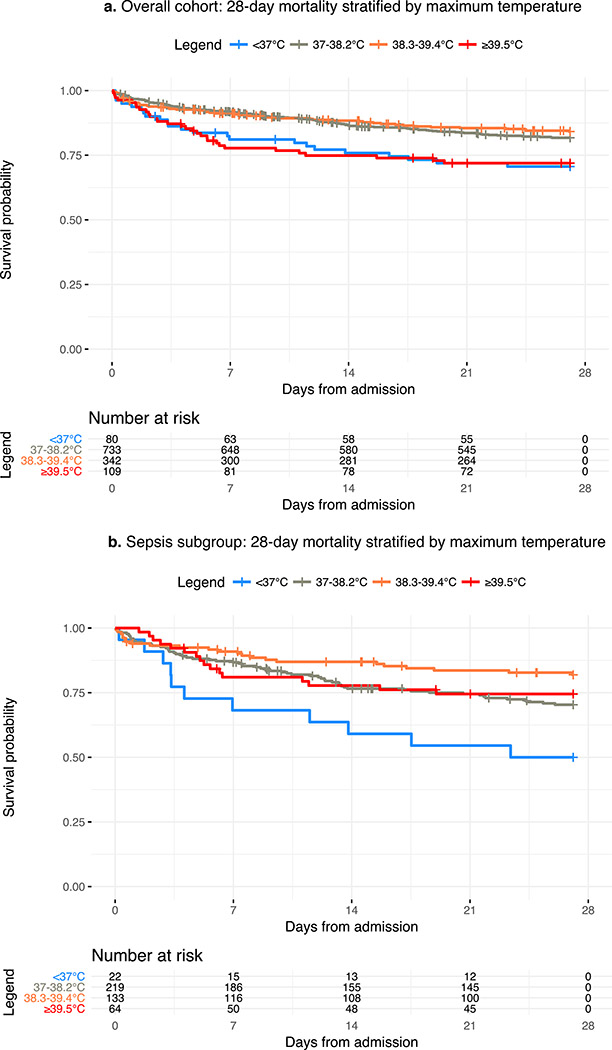
Methods: This is a retrospective cohort study of 1,264 patients requiring mechanical ventilation initiated in the ED with subsequent admission to an intensive care unit. Maximum body temperature was recorded for the first 24 h after ED admission and categorized into four categories: <37°C, 37°C to 38.2°C, 38.3°C to 39.4°C, and ≥39.5°C. The primary outcome was 28-day mortality. We conducted a planned subgroup analysis of patients with sepsis at the time of intubation. Multivariable Cox proportional hazard ratios (HRs) were used to assess the relationship between temperature, antipyretics, and mortality.
Results: Multivariable Cox proportional HRs demonstrated that a maximum temperature ≥39.5°C was associated with increased mortality (adjusted hazard ratio [aHR] 1.59 [95% confidence interval, CI, 1.05-2.39]). In the subgroup of patients with sepsis, a maximum temperature of 38.3°C to 39.4°C was associated with survival (aHR 0.61 [95% CI, 0.39-0.99]). There was no difference in 28-day mortality between patients who did and did not receive antipyretic medication in either the overall cohort or the septic subgroup.
Conclusion: High fever (≥39.5°C) was associated with increased risk for mortality in mechanically ventilated patients. However, in patients with sepsis, moderate fever (38.3°C-39.4°C) was protective. Antipyretic medication was not associated with changes in outcome. This suggests that fever may have different implications in septic versus nonseptic mechanically ventilated patients.
Figures
References
-
- Easter BD, Fischer C, Fisher J: The use of mechanical ventilation in the ED. Am J Emerg Med 30:1183–1188, 2012. - PubMed
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM: The epidemiology of mechanical ventilation use in the United States*. Crit Care Med 38:1947–1953, 2010. - PubMed
-
- Ashbaugh D, Boyd Bigelow D, Petty T, Levine B: ACUTE RESPIRATORY DISTRESS IN ADULTS. Lancet 290:319–323, 1967. - PubMed
-
- Ware LB, Matthay MA: The Acute Respiratory Distress Syndrome. N Engl J Med 342:1334–1349, 2000. - PubMed
-
- Ricard J-D, Dreyfuss D, Saumon G: Ventilator-induced lung injury. Curr Opin Crit Care 8:12–20, 2002. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
