

Cardiovascular Organ Damage and Blood Pressure Levels Predict Adverse Events in Multiple Myeloma Patients Undergoing Carfilzomib Therapy
- PMID: 31058856
- PMCID: PMC6562621
- DOI: 10.3390/cancers11050622
Cardiovascular Organ Damage and Blood Pressure Levels Predict Adverse Events in Multiple Myeloma Patients Undergoing Carfilzomib Therapy
Abstract
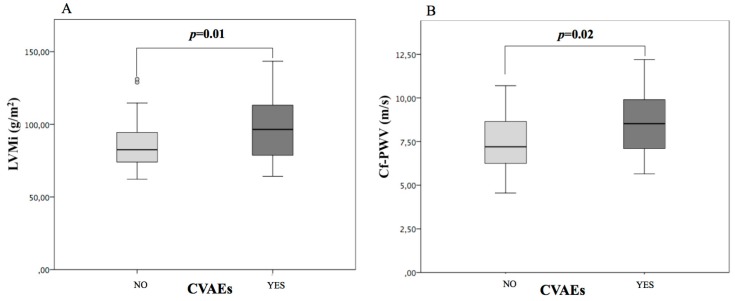
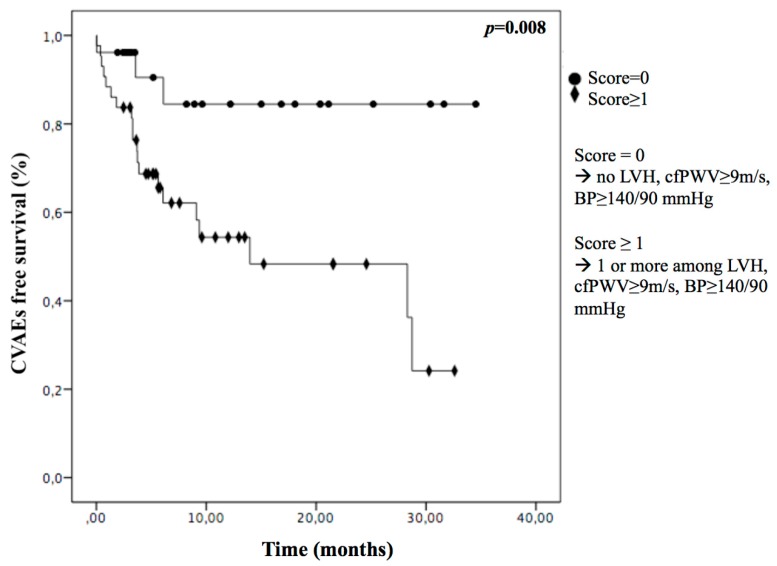
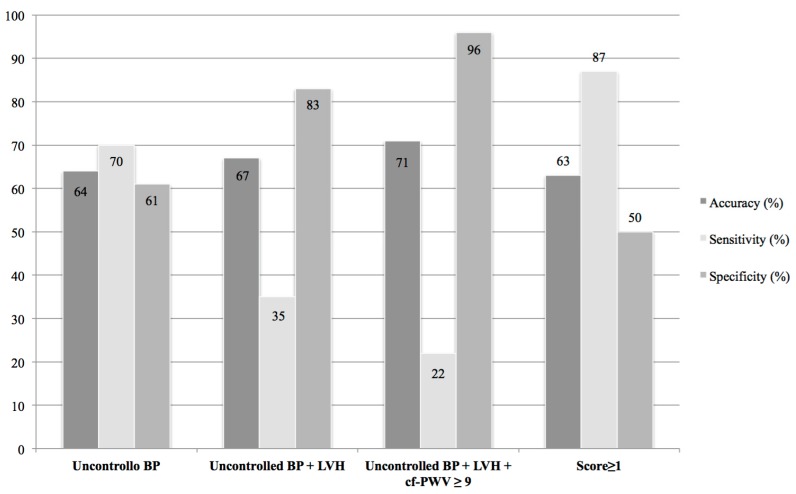
Carfilzomib is a second-generation proteasome inhibitor approved for the treatment of multiple myeloma (MM). It seems to determine cardiovascular toxicity, primarily arterial hypertension. No predictive factors for cardiovascular adverse events (CVAEs) are known in patients affected by multiple myeloma treated with carfilzomib. We evaluated the role of cardiovascular organ damage parameters to predict CVAEs in MM patients taking carfilzomib. Seventy patients affected by MM were prospectively enrolled. A comprehensive cardiovascular evaluation was performed before carfilzomib therapy; they underwent a transthoracic echocardiogram and the assessment of carotid-femoral pulse wave velocity. All the patients were followed up (FU) to determine the incidence of CVAEs. The mean age was 60.3 ± 8.2, and 51% were male. The median FU was 9.3 (4.3; 20.4) months. A proportion of 33% experienced CVAEs, 91% of them had uncontrolled hypertension, 4.5% acute coronary syndrome, and 4.5% cardiac arrhythmias. Subjects with CVAEs after carfilzomib treatment had significantly higher blood pressure values, left ventricular mass (98 ± 23 vs. 85 ± 17 g/m2, p = 0.01), and pulse wave velocity (8.5 ± 1.7 vs. 7.5 ± 1.6 m/s, p = 0.02) at baseline evaluation compared to the others. Furthermore, baseline uncontrolled blood pressure, left ventricular hypertrophy, and pulse wave velocity ≥ 9 m/s were able to identify patients at higher risk of developing CVAEs during FU. These preliminary findings indicate that blood pressure control, left ventricular mass, and pulse wave velocity may predict CVAEs in MM patients treated with carfilzomib.
Keywords: arterial hypertension; cardio-toxicity; cardiovascular adverse event; cardiovascular organ damage; multiple myeloma.
Conflict of interest statement
A.M. received honoraria for Advisory board from Amgen and Janssen S.B.: she has received honoraria from Jannsen, Amgen, Celgene and BMS; Advisory board for Amgen and Janssen. F.G.: she has received honoraria from Jannsen, Amgen, Takeda, Celgene and BMS; Advisory board for Jannsen, Amgen, Takeda, Celgene, BMS and Roche. The other authors declare no conflict of interest.
Figures
References
-
- Dimopoulos M.A., Goldschmidt H., Niesvizky R., Joshua D., Chng W.J., Oriol A., Orlowski R.Z., Ludwig H., Facon T., Hajek R., et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): An interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18:1327–1337. doi: 10.1016/S1470-2045(17)30578-8. - DOI - PubMed
-
- Dimopoulos M.A., Stewart A.K., Masszi T., Spicka I., Oriol A., Hajek R., Rosinol L., Siegel D., Mihaylov G.G., Goranova-Marinova V., et al. Carfilzomib-lenalidomide-dexamethasone vs. lenalidomide-dexamethasone in relapsed multiple myeloma by previous treatment. Blood Cancer J. 2017;7:e554. doi: 10.1038/bcj.2017.31. - DOI - PMC - PubMed
-
- Hajek R., Masszi T., Petrucci M.T., Palumbo A., Rosinol L., Nagler A., Yong K.L., Oriol A., Minarik J., Pour L., et al. A randomized phase III study of carfilzomib vs. low-dose corticosteroids with optional cyclophosphamide in relapsed and refractory multiple myeloma (FOCUS) Leukemia. 2017;31:107–114. doi: 10.1038/leu.2016.176. - DOI - PMC - PubMed
-
- Waxman A.J., Clasen S., Hwang W.T., Garfall A., Vogl D.T., Carver J., O’Quinn R., Cohen A.D., Stadtmauer E.A., Ky B., et al. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol. 2017;4:e174519. doi: 10.1001/jamaoncol.2017.4519. - DOI - PMC - PubMed
