

Effect of a Quality Improvement Intervention on Adherence to Therapies for Patients With Acute Ischemic Stroke and Transient Ischemic Attack: A Cluster Randomized Clinical Trial
- PMID: 31058947
- PMCID: PMC6692700
- DOI: 10.1001/jamaneurol.2019.1012
Effect of a Quality Improvement Intervention on Adherence to Therapies for Patients With Acute Ischemic Stroke and Transient Ischemic Attack: A Cluster Randomized Clinical Trial
Abstract
Importance: Translating evidence into clinical practice in the management of acute ischemic stroke (AIS) and transient ischemic attack (TIA) is challenging, especially in low- and middle-income countries.
Objective: To assess the effect of a multifaceted quality improvement intervention on adherence to evidence-based therapies for care of patients with AIS and TIA.
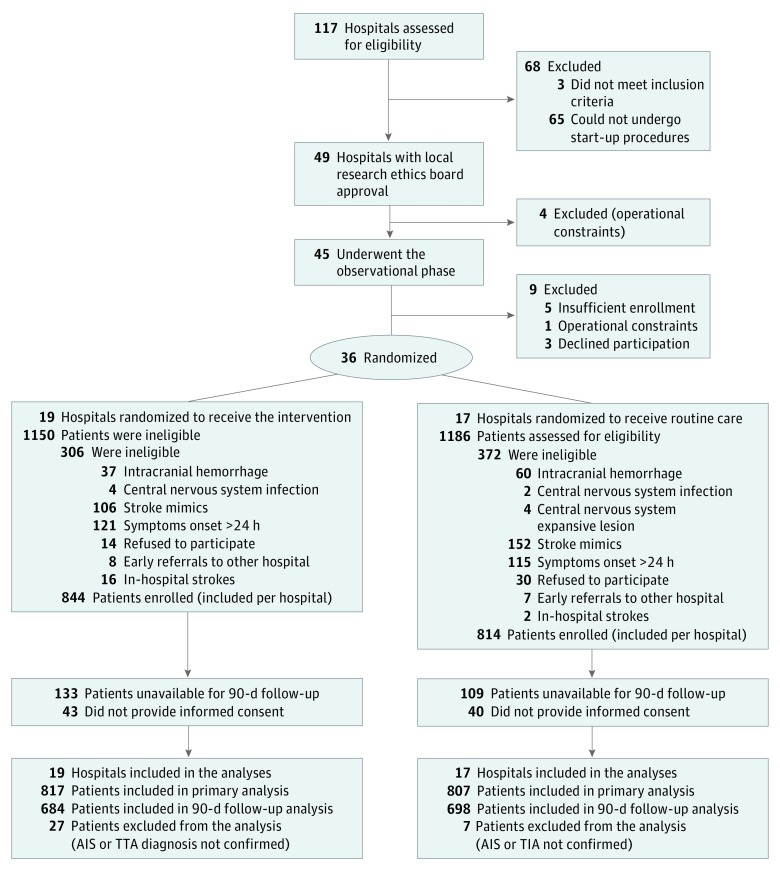
Design, setting and participants: This 2-arm cluster-randomized clinical trial assessed 45 hospitals and 2336 patients with AIS and TIA for eligibility before randomization. Eligible hospitals were able to provide care for patients with AIS and TIA in Brazil, Argentina, and Peru. Recruitment started September 12, 2016, and ended February 26, 2018; follow-up ended June 29, 2018. Data were analyzed using the intention-to-treat principle.
Interventions: The multifaceted quality improvement intervention included case management, reminders, a roadmap and checklist for the therapeutic plan, educational materials, and periodic audit and feedback reports to each intervention cluster.
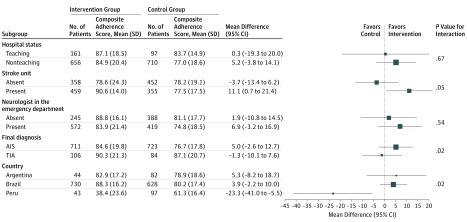
Main outcomes and measures: The primary outcome was a composite adherence score for AIS and TIA performance measures. Secondary outcomes included an all-or-none composite end point of performance measures, the individual process measure components of the composite end points, and clinical outcomes at 90 days after admission (stroke recurrence, death, and disability measured by the modified Rankin scale).
Results: A total of 36 hospitals and 1624 patients underwent randomization. Nineteen hospitals were randomized to the quality improvement intervention and 17 to routine care. The overall mean (SD) age of patients enrolled in the study was 69.4 (13.5) years, and 913 (56.2%) were men. Overall mean (SD) composite adherence score for the 10 performance measures in the intervention group hospitals compared with control group hospitals was 85.3% (20.1%) vs 77.8% (18.4%) (mean difference, 4.2%; 95% CI, -3.8% to 12.2%). As a secondary end point, 402 of 817 patients (49.2%) at intervention hospitals received all the therapies that they were eligible for vs 203 of 807 (25.2%) in the control hospitals (odds ratio, 2.59; 95% CI, 1.22-5.53; P = .01).
Conclusions and relevance: A multifaceted quality improvement intervention did not result in a significant increase in composite adherence score for evidence-based therapies in patients with AIS or TIA. However, when using an all-or-none approach, the intervention resulted in improved adherence to evidence-based therapies.
Trial registration: ClinicalTrials.gov identifier: NCT02223273.
Conflict of interest statement
Figures
References
-
- GBD 2016 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1260-1344. doi:10.1016/S0140-6736(17)32130-X - DOI - PMC - PubMed
-
- Lees KR, Bluhmki E, von Kummer R, et al. ; ECASS, ATLANTIS, NINDS and EPITHET rt-PA Study Group . Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375(9727):1695-1703. doi:10.1016/S0140-6736(10)60491-6 - DOI - PubMed
-
- Emberson J, Lees KR, Lyden P, et al. ; Stroke Thrombolysis Trialists’ Collaborative Group . Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929-1935. doi:10.1016/S0140-6736(14)60584-5 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
