

Fractures and Subsequent Graft Loss and Mortality among Older Kidney Transplant Recipients
- PMID: 31059126
- PMCID: PMC6684377
- DOI: 10.1111/jgs.15962
Fractures and Subsequent Graft Loss and Mortality among Older Kidney Transplant Recipients
Abstract
Objectives: Older adults who undergo kidney transplantation (KT) are living longer with a functioning graft and are at risk for age-related adverse events including fractures. Understanding recipient, transplant, and donor factors and the outcomes associated with fractures may help identify older KT recipients at increased risk. We determined incidence of hip, vertebral, and extremity fractures; assessed factors associated with incident fractures; and estimated associations between fractures and subsequent death-censored graft loss (DCGL) and mortality.
Design: This was a prospective cohort study of patients who underwent their first KT between January 1, 1999, and December 31, 2014.
Setting: We linked data from the Scientific Registry of Transplant Recipients to Medicare claims through the US Renal Data System.
Participants: The analytic population included 47 815 KT recipients aged 55 years or older.
Measurements: We assessed the cumulative incidence of and factors associated with post-KT fractures (hip, vertebral, or extremity) using competing risks models. We estimated risk of DCGL and mortality after fracture using adjusted Cox proportional hazards models.
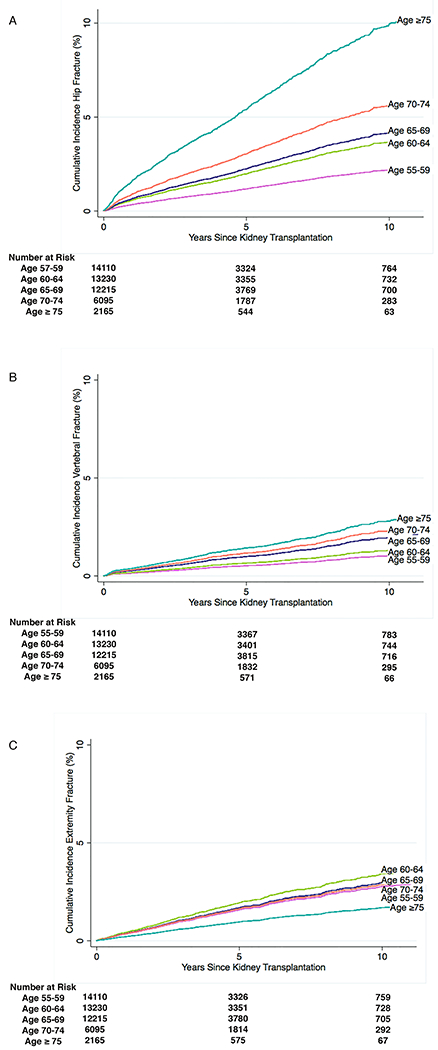
Results: The 5-year incidence of post-KT hip, vertebral, and extremity fracture for those aged 65 to 69 years was 2.2%, 1.0%, and 1.7%, respectively. Increasing age was associated with higher hip (adjusted hazard ratio [aHR] = 1.37 per 5-y increase; 95% confidence interval [CI] = 1.30-1.45) and vertebral (aHR = 1.31; 95% CI = 1.20-1.42) but not extremity (aHR = .97; 95% CI = .91-1.04) fracture risk. DCGL risk was higher after hip (aHR = 1.34; 95% CI = 1.12-1.60) and extremity (aHR = 1.30; 95% CI = 1.08-1.57) fracture. Mortality risk was higher after hip (aHR = 2.31; 95% CI = 2.11-2.52), vertebral (aHR = 2.80; 95% CI = 2.44-3.21), and extremity (aHR = 1.85; 95% CI = 1.64-2.10) fracture.
Conclusion: Our findings suggest that older KT recipients are at higher risk for hip and vertebral fracture but not extremity fracture; and those with hip, vertebral, or extremity fracture are more likely to experience subsequent graft loss or mortality. These findings underscore that different fracture types may have different underlying etiologies and risks, and they should be approached accordingly. J Am Geriatr Soc 67:1680-1688, 2019.
Keywords: fractures; graft loss; kidney transplant; mortality; older adults.
© 2019 The American Geriatrics Society.
Conflict of interest statement
Conflict of Interest
D.L.S holds speaking honoraria from Sanofi, Novartis, and CSL Behring. The remaining authors of this manuscript have no conflicts of interest to disclose.
Figures
References
-
- Knoll GA. Kidney transplantation in the older adult. Am J Kidney Dis 2013;61(5):790–797. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DK120518/DK/NIDDK NIH HHS/United States
- R01DK114074/DK/NIDDK NIH HHS/United States
- K01AG043501/AG/NIA NIH HHS/United States
- R01AG042504/NH/NIH HHS/United States
- K24DK101828/NH/NIH HHS/United States
- R01AG055781/AG/NIA NIH HHS/United States
- K24 AI144954/AI/NIAID NIH HHS/United States
- K24 DK101828/DK/NIDDK NIH HHS/United States
- P30AG021334/AG/NIA NIH HHS/United States
- P30 AG021334/AG/NIA NIH HHS/United States
- K01 AG043501/AG/NIA NIH HHS/United States
- R01DK120518/NH/NIH HHS/United States
- R01 AG055781/AG/NIA NIH HHS/United States
- R01 AG042504/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
