

Pose Estimation of Periacetabular Osteotomy Fragments With Intraoperative X-Ray Navigation
- PMID: 31059424
- PMCID: PMC7297497
- DOI: 10.1109/TBME.2019.2915165
Pose Estimation of Periacetabular Osteotomy Fragments With Intraoperative X-Ray Navigation
Abstract
Objective: State-of-the-art navigation systems for pelvic osteotomies use optical systems with external fiducials. In this paper, we propose the use of X-ray navigation for pose estimation of periacetabular fragments without fiducials.
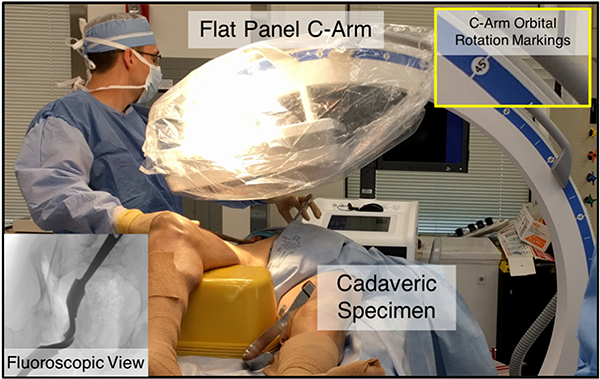
Methods: A two-dimensional/three-dimensional (2-D/3-D) registration pipeline was developed to recover fragment pose. This pipeline was tested through an extensive simulation study and six cadaveric surgeries. Using osteotomy boundaries in the fluoroscopic images, the preoperative plan was refined to more accurately match the intraoperative shape.
Results: In simulation, average fragment pose errors were 1.3 ° /1.7 mm when the planned fragment matched the intraoperative fragment, 2.2 ° /2.1 mm when the plan was not updated to match the true shape, and 1.9 ° /2.0 mm when the fragment shape was intraoperatively estimated. In cadaver experiments, the average pose errors were 2.2 ° /2.2 mm, 3.8 ° /2.5 mm, and 3.5 ° /2.2 mm when registering with the actual fragment shape, a preoperative plan, and an intraoperatively refined plan, respectively. Average errors of the lateral center edge angle were less than 2 ° for all fragment shapes in simulation and cadaver experiments.
Conclusion: The proposed pipeline is capable of accurately reporting femoral head coverage within a range clinically identified for long-term joint survivability.
Significance: Human interpretation of fragment pose is challenging and usually restricted to rotation about a single anatomical axis. The proposed pipeline provides an intraoperative estimate of rigid pose with respect to all anatomical axes, is compatible with minimally invasive incisions, and has no dependence on external fiducials.
Figures





References
-
- Murphy SB, Ganz R, and Müller M, “The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome,” J. Bone Joint Surg. Amer, vol. 77, no. 7, pp. 985–989, 1995. - PubMed
-
- Ganz R et al., “A new periacetabular osteotomy for the treatment of hip dysplasias technique and preliminary results,” Clin. Orthopaedics Related Res, vol. 232, pp. 26–36, 1988. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
