

Pathogenesis of Acute Respiratory Distress Syndrome
- PMID: 31060086
- PMCID: PMC7060969
- DOI: 10.1055/s-0039-1683996
Pathogenesis of Acute Respiratory Distress Syndrome
Abstract
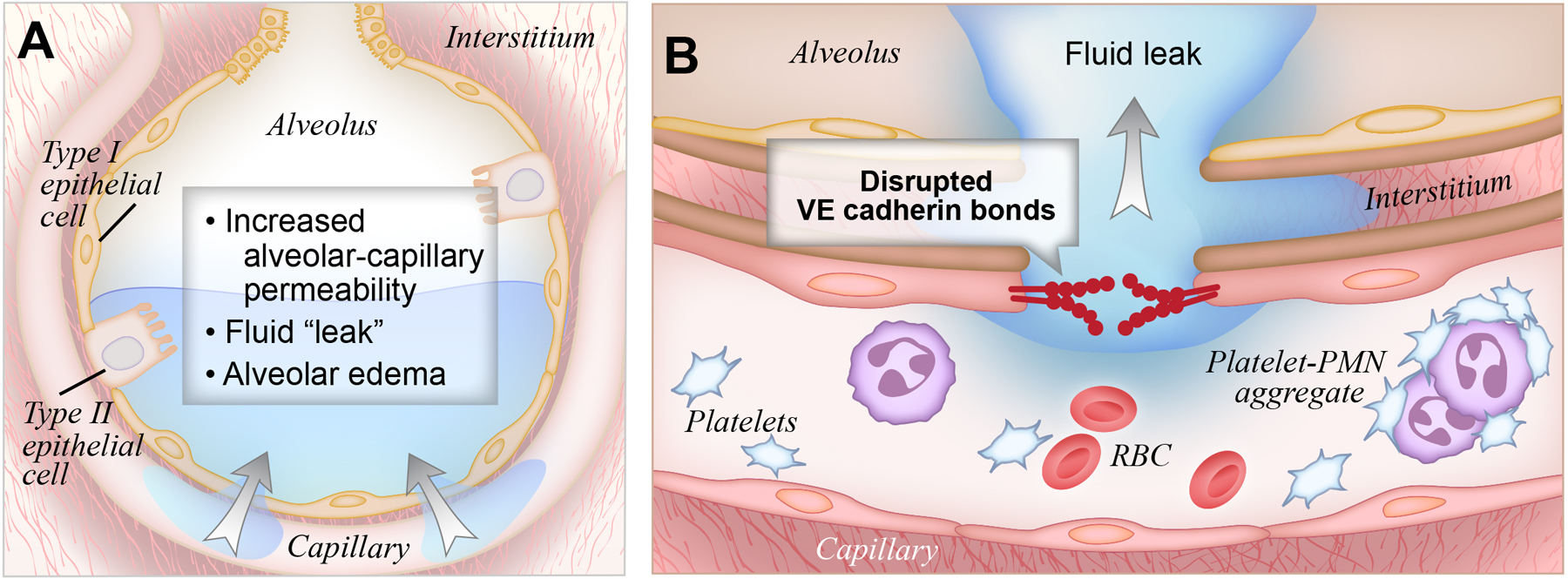
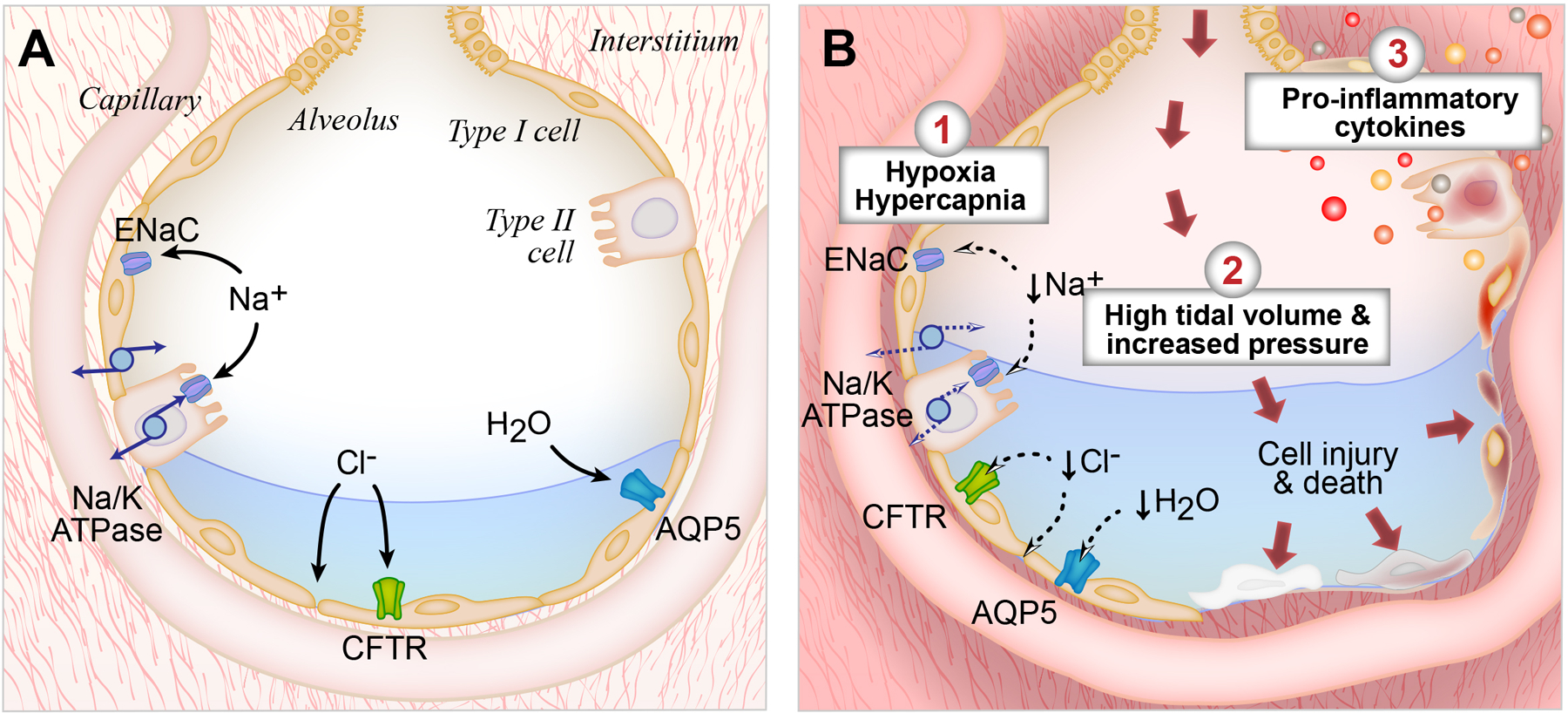
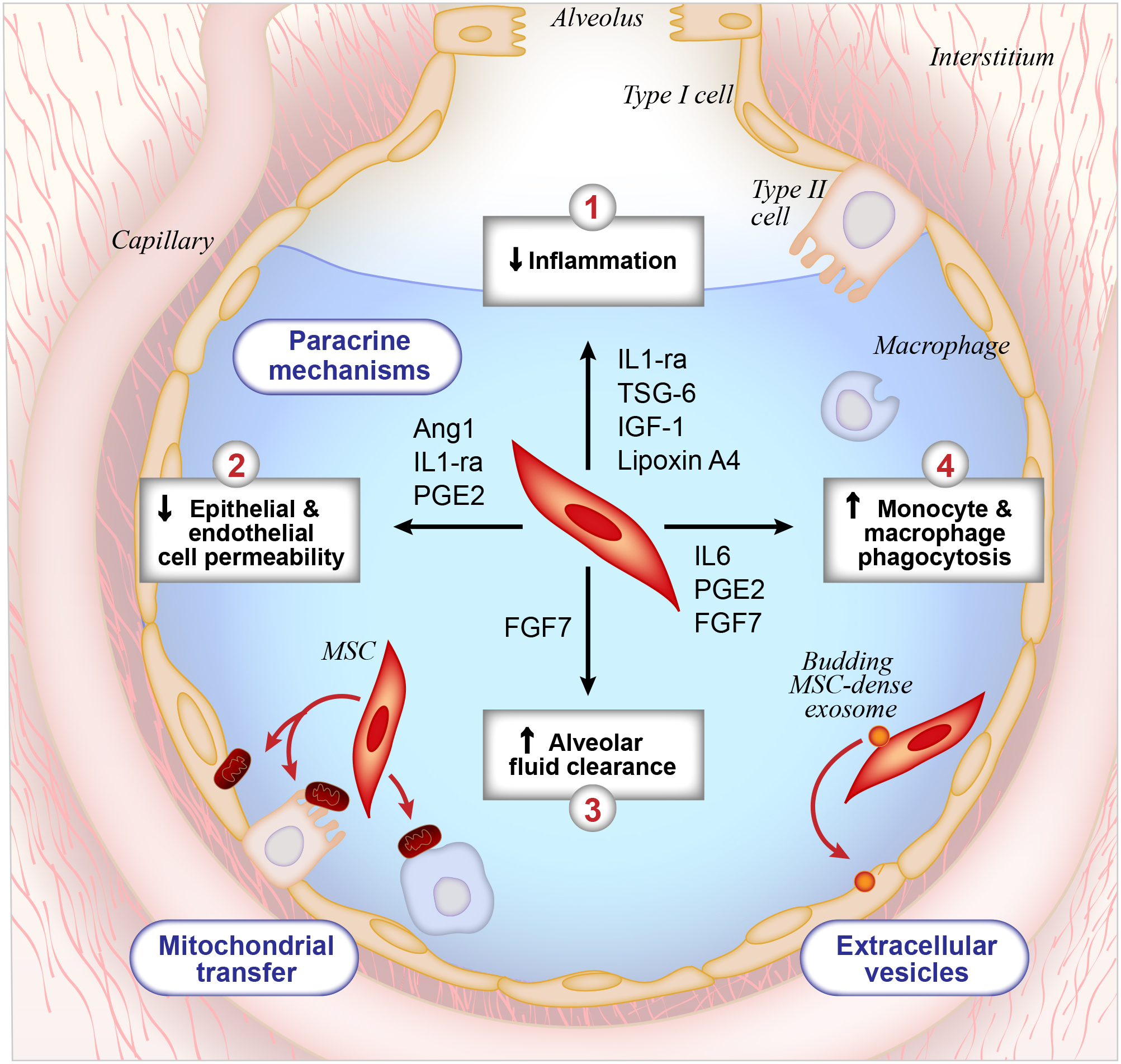
Acute respiratory distress syndrome (ARDS) is a syndrome of acute respiratory failure caused by noncardiogenic pulmonary edema. Despite five decades of basic and clinical research, there is still no effective pharmacotherapy for this condition and the treatment remains primarily supportive. It is critical to study the molecular and physiologic mechanisms that cause ARDS to improve our understanding of this syndrome and reduce mortality. The goal of this review is to describe our current understanding of the pathogenesis and pathophysiology of ARDS. First, we will describe how pulmonary edema fluid accumulates in ARDS due to lung inflammation and increased alveolar endothelial and epithelial permeabilities. Next, we will review how pulmonary edema fluid is normally cleared in the uninjured lung, and describe how these pathways are disrupted in ARDS. Finally, we will explain how clinical trials and preclinical studies of novel therapeutic agents have further refined our understanding of this condition, highlighting, in particular, the study of mesenchymal stromal cells in the treatment of ARDS.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Conflict of interest statement
This work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ferguson ND, Fan E, Camporota L, Antonelli M, Anzueto A, Beale R, Brochard L, Brower R, Esteban A, Gattinoni L, Rhodes A. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive care medicine 2012;38:1573–82. - PubMed
-
- Villar J, Blanco J, Kacmarek RM. Current incidence and outcome of the acute respiratory distress syndrome. Current opinion in critical care 2016;22:1–6. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern EJ, Hudson LD. Incidence and outcomes of acute lung injury. New England Journal of Medicine 2005;353:1685–93. - PubMed
-
- Máca J, Jor O, Holub M, Sklienka P, Burša F, Burda M, Janout V, Ševčík P. Past and present ARDS mortality rates: a systematic review. Respiratory care 2017;62:113–22. - PubMed
