

The neuropsychological phenotype of Chediak-Higashi disease
- PMID: 31060595
- PMCID: PMC6503440
- DOI: 10.1186/s13023-019-1049-x
The neuropsychological phenotype of Chediak-Higashi disease
Abstract
Background/objectives: Chediak-Higashi Disease (CHD) is a rare autosomal disorder, purported to have cognitive and neurological impairments. Prior descriptions of cognitive impairment, however, are solely based on subjective, unstructured observations rather than on formal neuropsychological measures.
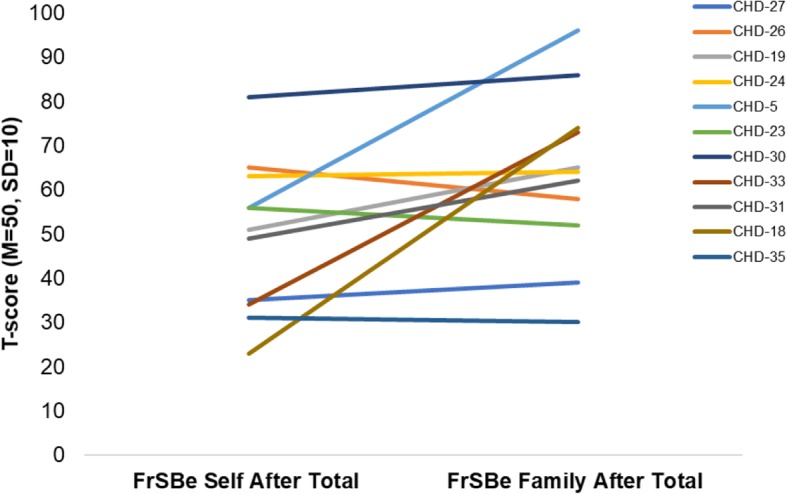
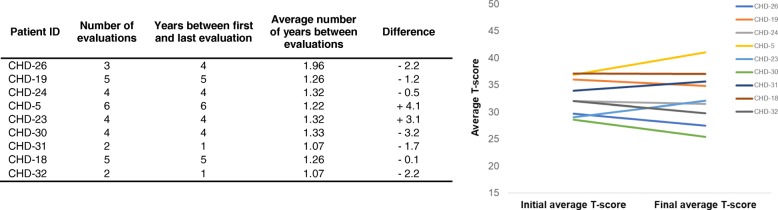
Methods: Four pediatric and 14 adult patients with diagnostically confirmed CHD were administered a neuropsychological battery assessing memory, attention, processing speed, psychomotor speed, language fluency, executive function, and general intelligence. Nine of the adult patients received follow-up evaluations to elucidate the longitudinal progression or stability of cognition over time.
Results: Pediatric CHD patients performed within the average range. Adult patients, however, performed below average on nearly all measures administered, and endorsed subjective reports of learning difficulties and poor academic performance in childhood. In particular, patients struggled with memory and psychomotor speed tasks, with 75% or more of patients scoring in the bottom 2.3 percentile in these two domains. No significant declines in cognition were observed among the patients who completed follow-up evaluations (M = 39.90, SD = 8.03 months between visits). Exploratory analyses suggested that adult patients who had classic CHD and previously received bone marrow transplants (BMTs; n = 3) exhibited moderately greater cognitive impairment than adult patients who had atypical CHD and had not received BMTs (n = 10).
Conclusions: Adult patients with CHD uniformly exhibit deficits in multiple domains, but in psychomotor speed and memory, in particular. Based on their neuropsychological profile, their ability to hold jobs and succeed in school may require support and special accommodations. The source of cognitive deficits is probably multifactorial including central nervous system involvement in CHD, and, for those transplanted, BMT-related side effects and complications. Absence of cognitive decline at three-year follow-up is encouraging but does not exclude progression at a slower time-scale. Future work should elucidate the possible effects and timing of BMT on cognition, as well as the mechanisms driving neuropsychological impairment in CHD.
Keywords: Bone marrow transplant; Chediak-Higashi disease; Intellectual disability; Neuropsychology.
Conflict of interest statement
Ethics approval and consent to participate
The present study was approved by the National Human Genome Research Institute IRB. Informed consent was obtained from either patients themselves or their legal guardians prior to study participation.
Consent for publication
Not applicable.
Competing interests
All authors declare they have no competing interests to disclose. The opinions expressed in the article are the views of the authors and do not reflect the views of the Department of Health and Human Services or the United States government.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Haddad E, Le Deist F, Blanche S, et al. Treatment of Chediak-Higashi syndrome by allogenic bone marrow transplantation: report of 10 cases. Blood. 1995;85:3328–3333. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
