

Diagnosing celiac disease: A critical overview
- PMID: 31060993
- PMCID: PMC6505646
- DOI: 10.5152/tjg.2018.18635
Diagnosing celiac disease: A critical overview
Abstract
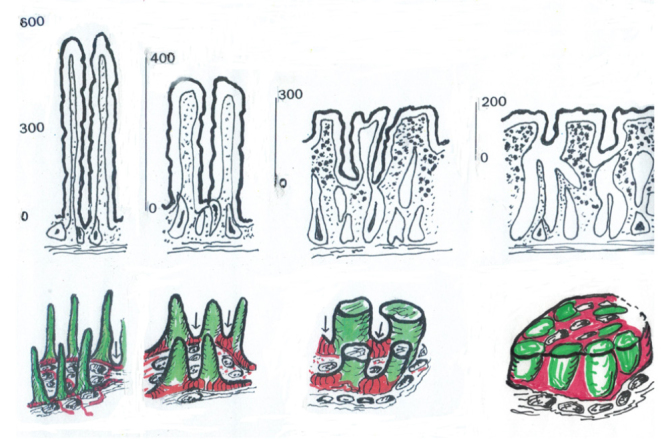
The diagnosis of celiac disease (CD) no longer rests on a malabsorptive state or severe mucosal lesions. For the present, diagnosis will always require the gold-standard of a biopsy, interpreted through its progressive phases (Marsh classification). Marsh classification articulated the immunopathological spectrum of gluten-induced mucosal changes in association with the recognition of innate (Marsh I infiltration) and T cell-based adaptive (Marsh II, and the surface re-organisation typifying Marsh III lesions) responses. Through the Marsh classification the diagnostic goalposts were considerably widened thus, over its time-course, permitting countless patients to begin a gluten-free diet but who, on previous criteria, would have been denied such vital treatment. The revisions of this classification failed to provide additional insight in the interpretation of mucosal pathology. Morever, the subclassification of Marsh 3 imposed an enormous amount of extra work on pathologists with no aid in diagnosis, treatment, or prognosis. Therefore, it should now be apparent that if gastroenterologists ignore these sub-classifications in clinical decision-making, then on that basis alone, there is no need whatsoever for pathologists to persist in reporting them. Since new treatments are under critical assessment, we might have to consider use of some other higher level histological techniques sensitive enough to detect the changes sought. A promising alternative would be to hear more voices from imaginative histopathologists or morphologists together with some more insightful approaches, involving molecular-based techniques and stem cell research may be to evaluate mucosal pathology in CD.
Conflict of interest statement
Figures
References
-
- Menghini G. One-second needle biopsy of the liver. Gastroenterology. 1958;35:190–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical