

Genomic correlates of clinical outcome in advanced prostate cancer
- PMID: 31061129
- PMCID: PMC6561293
- DOI: 10.1073/pnas.1902651116
Genomic correlates of clinical outcome in advanced prostate cancer
Abstract
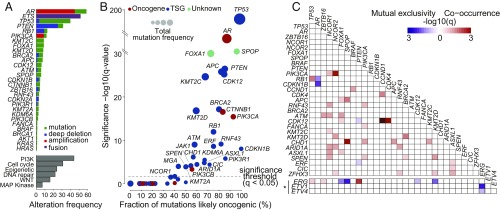
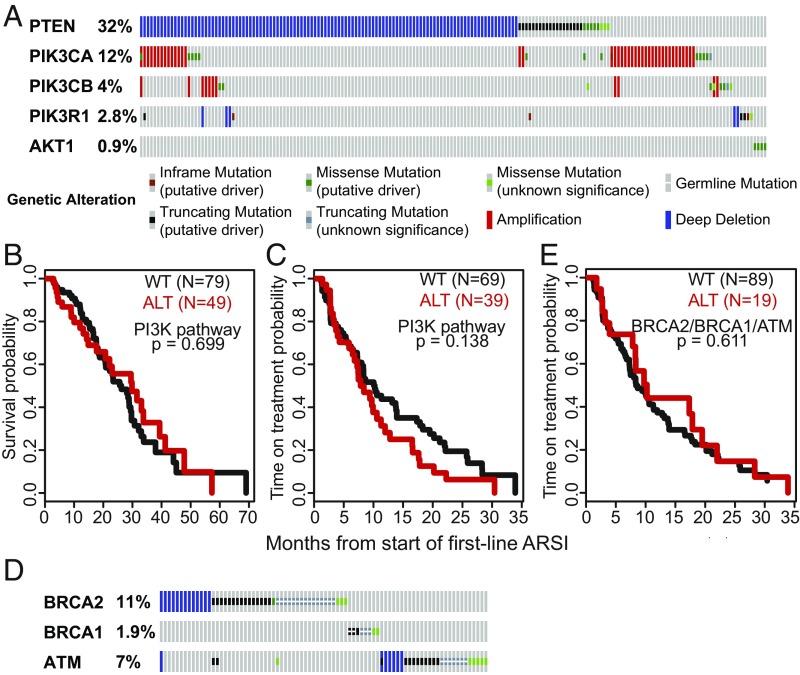
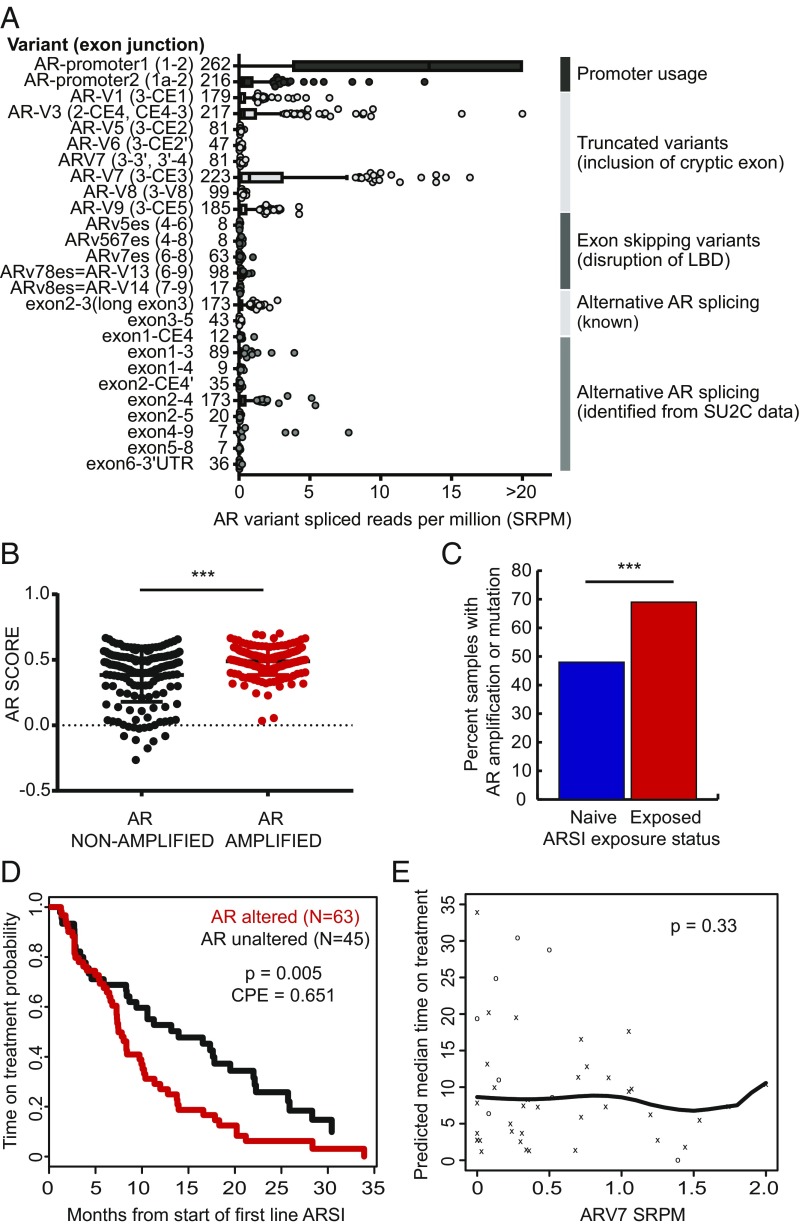
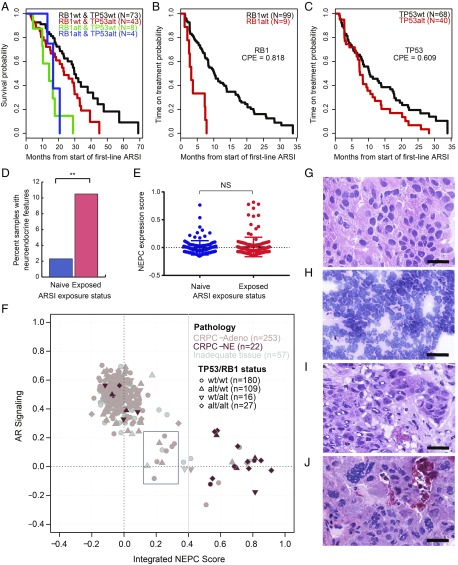
Heterogeneity in the genomic landscape of metastatic prostate cancer has become apparent through several comprehensive profiling efforts, but little is known about the impact of this heterogeneity on clinical outcome. Here, we report comprehensive genomic and transcriptomic analysis of 429 patients with metastatic castration-resistant prostate cancer (mCRPC) linked with longitudinal clinical outcomes, integrating findings from whole-exome, transcriptome, and histologic analysis. For 128 patients treated with a first-line next-generation androgen receptor signaling inhibitor (ARSI; abiraterone or enzalutamide), we examined the association of 18 recurrent DNA- and RNA-based genomic alterations, including androgen receptor (AR) variant expression, AR transcriptional output, and neuroendocrine expression signatures, with clinical outcomes. Of these, only RB1 alteration was significantly associated with poor survival, whereas alterations in RB1, AR, and TP53 were associated with shorter time on treatment with an ARSI. This large analysis integrating mCRPC genomics with histology and clinical outcomes identifies RB1 genomic alteration as a potent predictor of poor outcome, and is a community resource for further interrogation of clinical and molecular associations.
Keywords: biomarkers; castration-resistant prostate cancer; clinical outcomes; integrative genomics.
Copyright © 2019 the Author(s). Published by PNAS.
Conflict of interest statement
Conflict of interest statement: W.A. has consulted for Clovis Oncology, Janssen, ORIC Pharmaceuticals, and MORE Health; has received honorarium from Caret Healthcare; has received travel funds from Clovis Oncology, ORIC Pharmaceuticals, and GlaxoSmithKline; and has received research funding from AstraZeneca, Clovis Oncology, Zenith Epigenetics, and GlaxoSmithKline. G.H., received research funding from Janssen. J.A. is currently employed at AstraZeneca. E.M.V.A. has consulted for Tango Therapeutics, Genome Medical, Invitae, Illumina, Foresite Capital, and Dynamo; has received research support from Novartis and BMS; has equity in Tango Therapeutics, Genome Medical, Syapse, and Microsoft; has received travel reimbursement from Roche/Genentech; and is a coinventor of institutional patents filed on ERCC2 mutations and chemotherapy response, chromatin mutations and immunotherapy response, and methods for clinical interpretation. H.B. has received research funding from Millennium Pharmaceuticals, AbbVie/Stemcentrx, Astellas, Janssen, and Eli Lilly; and is a consultant/advisor for Sanofi Genzyme and Janssen. S.T. is a coinventor for University of Michigan patents on ETS fusion genes, and diagnostic field of use licensed to Hologic/Gen-Probe Inc., which has sublicensed rights to Roche/Ventana Medical Systems; is a consultant for and has received honoraria from Janssen, AbbVie, Sanofi, Almac Diagnostics, and Astellas/Medivation; has performed sponsored research from Astellas/Medivation and GenomeDx; and is an equity holder in and employee of Strata Oncology. J.M. has consulted for AstraZeneca and Janssen; and has received travel support or speaker fees from Astellas, AstraZeneca, Sanofi, and IPSEN. D.B. has received honoraria and travel support from Janssen. H.I.S. has consulted for Astellas, Ferring Pharmaceuticals, Janssen Biotech, Janssen Research and Development, Sanofi Aventis, Clovis Oncology, Merck, and WCG Oncology; is a member of the board of directors for Asterias Biotherapeutics; and has received research support from Illumina Inc., Innocrin, and Janssen. P.W.K. is a board member for Context Therapeutics LLC, has consulted for BIND Biosciences, BN Immunotherapeutics, DRGT, GE Healthcare, Janssen Pharmaceutica, Metamark, New England Research Institutes, OncoCellMDx, Progenity, Sanofi-Aventis, Seer Biosciences Inc., Tarveda Therapeutics, and Thermo Fisher Scientific; serves on data safety monitoring boards for Genentech/Roche and Merck & Co.; and has investment interest in Context Therapeutics, DRGT, Seer Biosciences, Placon, and Tarveda Therapeutics. M.-E.T. has consuled for Janssen. J.S.d. is an advisory board member for AstraZeneca, Astellas, Bayer, Boehringer Ingelheim, Genentech/Roche, Genmab, GSK, Janssen, Merck Serono, Merck Sharp & Dohme, Menarini/Silicon Biosystems, Orion, Pfizer, Sanofi Aventis, and Taiho; and his institution has received funding or other support from AstraZeneca, Astellas, Bayer, Genentech, GSK, Janssen, Merck Serono, MSD, Menarini/Silicon Biosystems, Orion, Sanofi Aventis, and Taiho. P.S.N. is a compensated advisor to Janssen, Astellas, and Roche. M.A.R. is a coinventor on a patent for Gene Fusion Prostate Cancer (Harvard/Michigan) and EZH2 (Michigan) in the area of diagnostics and therapeutics; is a coinventor on a patent filed by Cornell University on AURKA and SPOP mutations in the field of prostate cancer diagnostics; receives royalties on licensing agreements for these inventions; and receives research support from Janssen, Eli Lilly, Millenium, and Sanofi-Aventis. C.L.S. serves on the board of directors of Novartis; is a cofounder of ORIC Pharmaceuticals and coinventor of enzalutamide and apalutamide; is a science advisor to Agios, Beigene, Blueprint, Column Group, Foghorn, Housey Pharma, Nextech, KSQ, Petra, and PMV; and is a cofounder of Seragon, purchased by Genentech/Roche in 2014.
Figures

Comment in
-
Predicting clinical outcome of therapy-resistant prostate cancer.Proc Natl Acad Sci U S A. 2019 Jun 4;116(23):11090-11092. doi: 10.1073/pnas.1906812116. Epub 2019 May 21. Proc Natl Acad Sci U S A. 2019. PMID: 31113882 Free PMC article. No abstract available.
-
Re: Genomic Correlates of Clinical Outcome in Advanced Prostate Cancer.J Urol. 2019 Dec;202(6):1099-1098. doi: 10.1097/01.JU.0000585744.96190.0a. Epub 2019 Sep 18. J Urol. 2019. PMID: 31532289 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
