

Medication-Related Problems in Outpatients With Decompensated Cirrhosis: Opportunities for Harm Prevention
- PMID: 31061951
- PMCID: PMC6492469
- DOI: 10.1002/hep4.1334
Medication-Related Problems in Outpatients With Decompensated Cirrhosis: Opportunities for Harm Prevention
Abstract
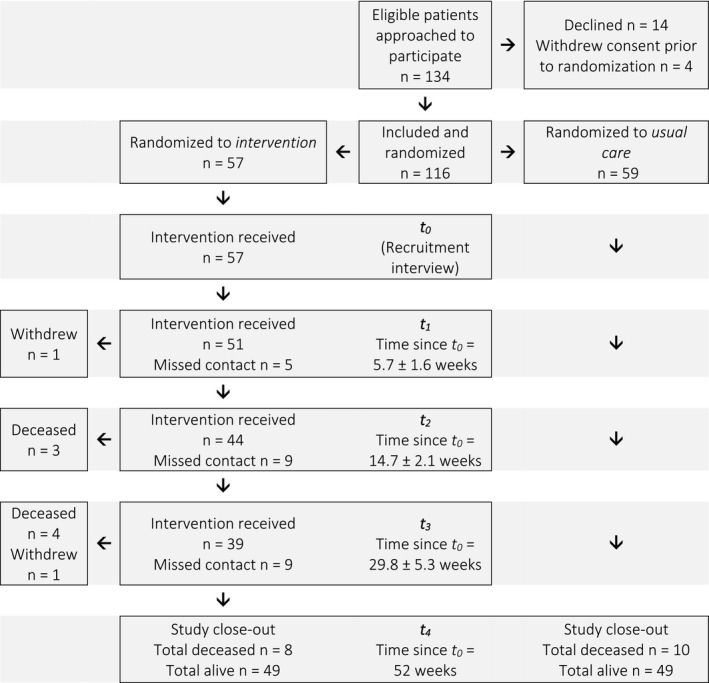
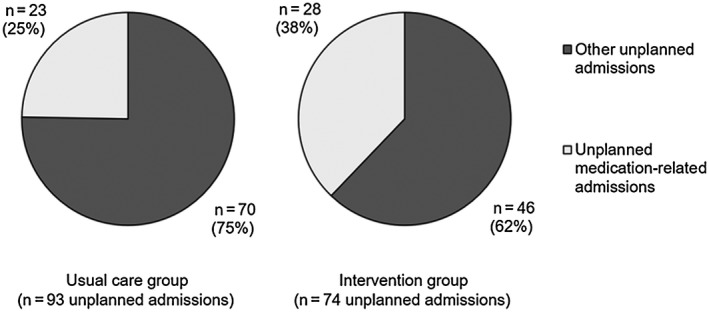
People with decompensated cirrhosis are often prescribed a complex regimen of therapeutic and prophylactic medications. In other chronic diseases, polypharmacy increases the risk of medication misadventure and medication-related problems (MRPs), with associated increased morbidity, mortality, and health care costs. This study examined MRPs in a cohort of ambulatory patients with a history of decompensated cirrhosis who were enrolled in a randomized controlled trial of a pharmacist-led, patient-oriented medication education intervention and assessed the association between MRPs and patient outcomes. A total of 375 MRPs were identified among 57 intervention patients (median, 6.0; interquartile range, 3.5-8.0 per patient; maximum 17). Nonadherence (31.5%) and indication issues (29.1%) were the most prevalent MRP types. The risk of potential harm associated with MRPs was low in 18.9% of instances, medium in 33.1%, and high in 48.0%, as categorized by a clinician panel using a risk matrix tool. Patients had a greater incidence rate of high-risk MRPs if they had a higher Child-Pugh score (incidence rate ratio [IRR], 1.31; 95% confidence interval [CI], 1.09-1.56); greater comorbidity burden (IRR, 1.15; 95% CI, 1.02-1.29); and were taking more medications (IRR, 1.12; 95% CI, 1.04-1.22). A total of 221 MRPs (58.9%) were resolved following pharmacist intervention. A greater proportion of high-risk MRPs were resolved compared to those of low and medium risk (68.9% versus 49.7%; P < 0.001). During the 12-month follow-up period, intervention patients had a lower incidence rate of unplanned admissions compared to usual care (IRR, 0.52; 95% CI, 0.30-0.92). Conclusion: High-risk MRPs are prevalent among adults with decompensated cirrhosis. Pharmacist intervention facilitated identification and resolution of high-risk MRPs and was associated with reduced incidence rate of unplanned hospital admissions in this group.
Figures
Comment in
-
Pharmacist-led educational interventions involving the "hidden" patient in cirrhosis-Caregivers.Hepatol Commun. 2022 Nov;6(11):3283. doi: 10.1002/hep4.1995. Epub 2022 May 26. Hepatol Commun. 2022. PMID: 35616305 Free PMC article. No abstract available.
References
-
- El‐Sherif O, Jiang ZG, Tapper EB, Huang KC, Zhong A, Osinusi A, et al. Basline factors associated with improvements in decompensated cirrhosis after direct‐acting antiviral therapy for hepatitis C virus infection. Gastroenterology 2018;154:2111‐2121. - PubMed
-
- Agrawal K, Kumar P, Markert R, Agrawal S. Risk factors for 30‐day readmissions of individuals with decompensated cirrhosis. South Med J 2015;108:682‐687. - PubMed
-
- Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm 1990;47:533‐543. - PubMed
LinkOut - more resources
Full Text Sources
