

Varicella in Tshuapa Province, Democratic Republic of Congo, 2009-2014
- PMID: 31062445
- PMCID: PMC8786670
- DOI: 10.1111/tmi.13243
Varicella in Tshuapa Province, Democratic Republic of Congo, 2009-2014
Abstract
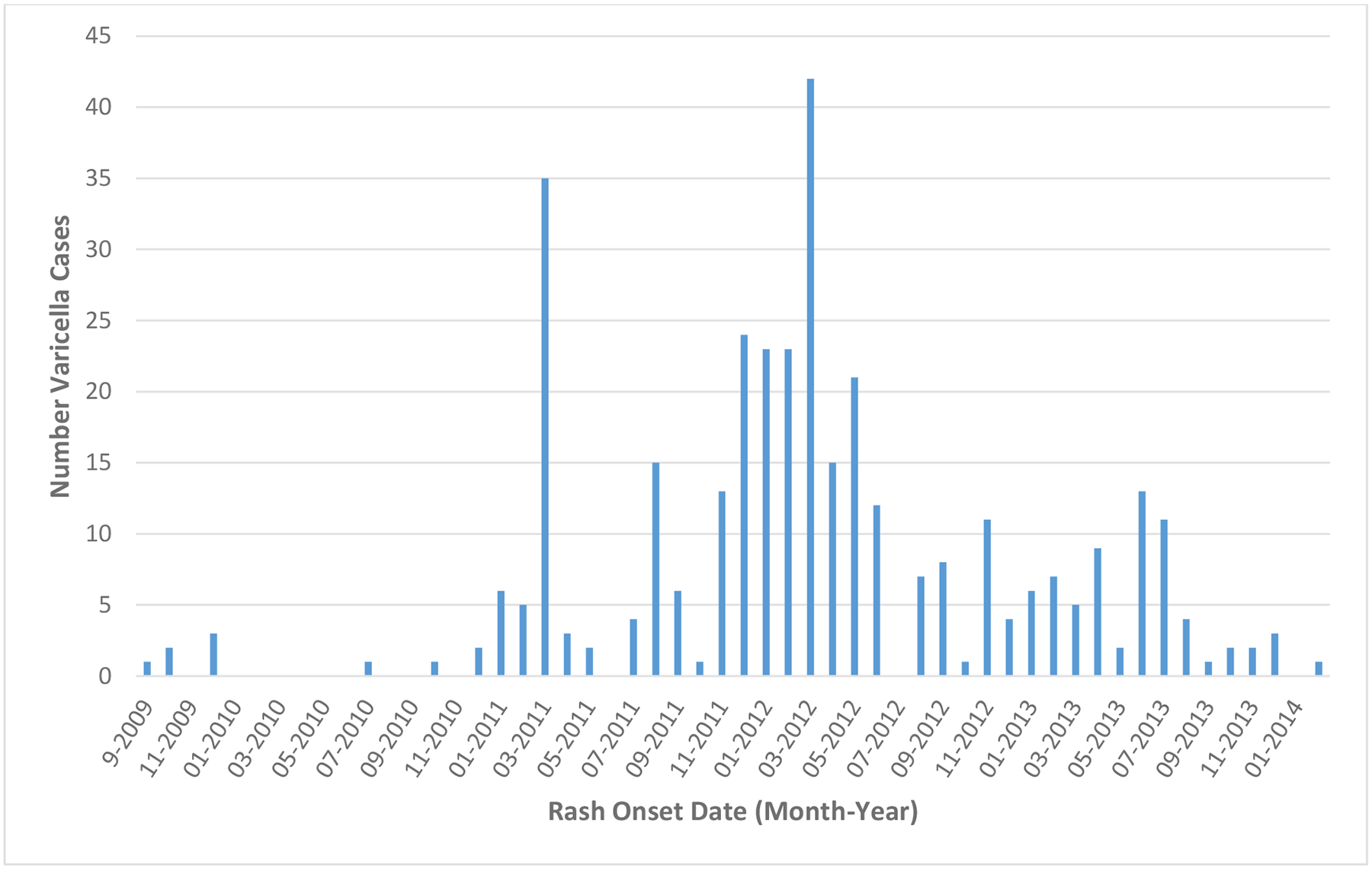
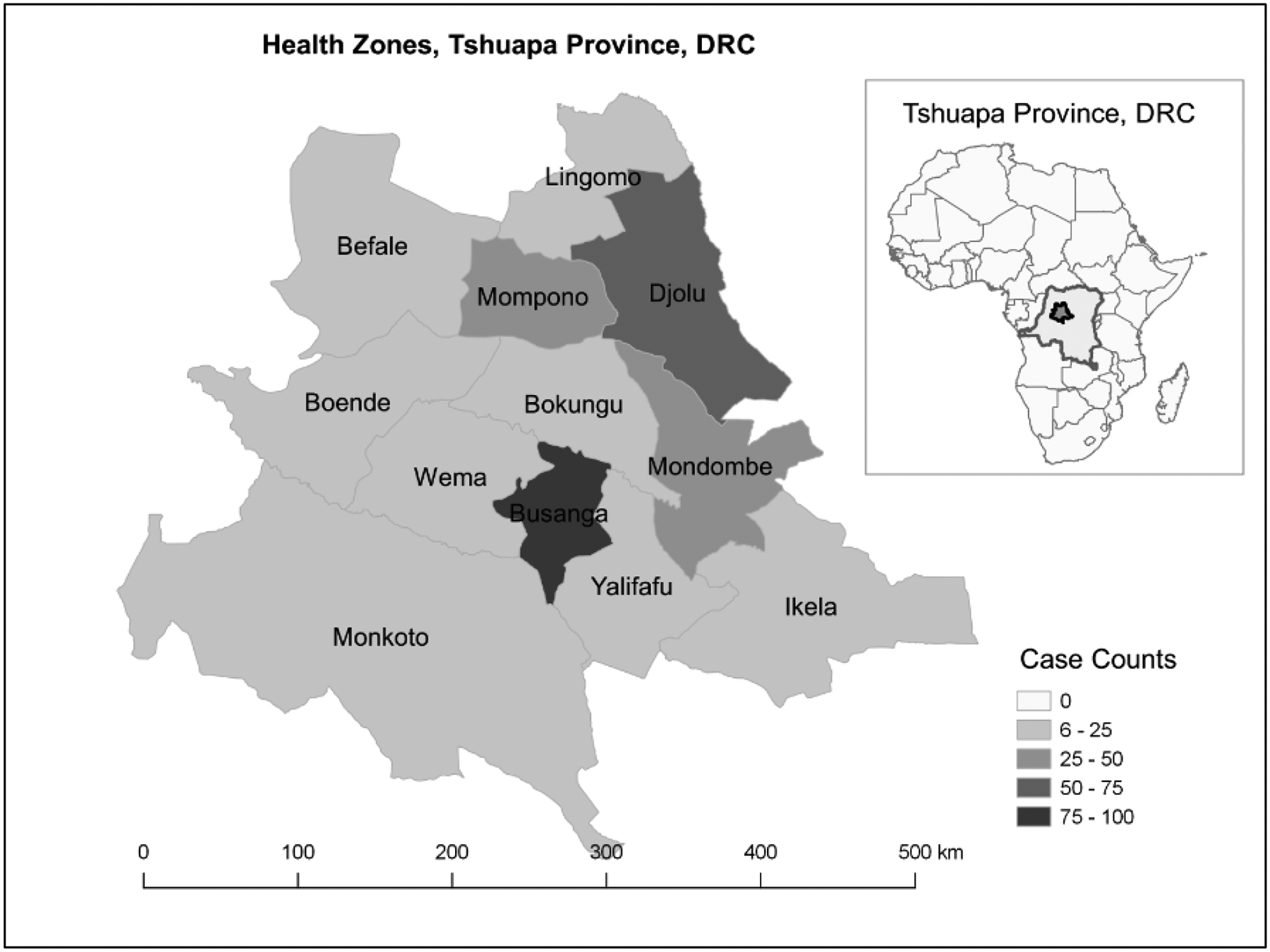
Objective: To describe varicella cases in Tshuapa Province of the Democratic Republic of the Congo identified during monkeypox surveillance.
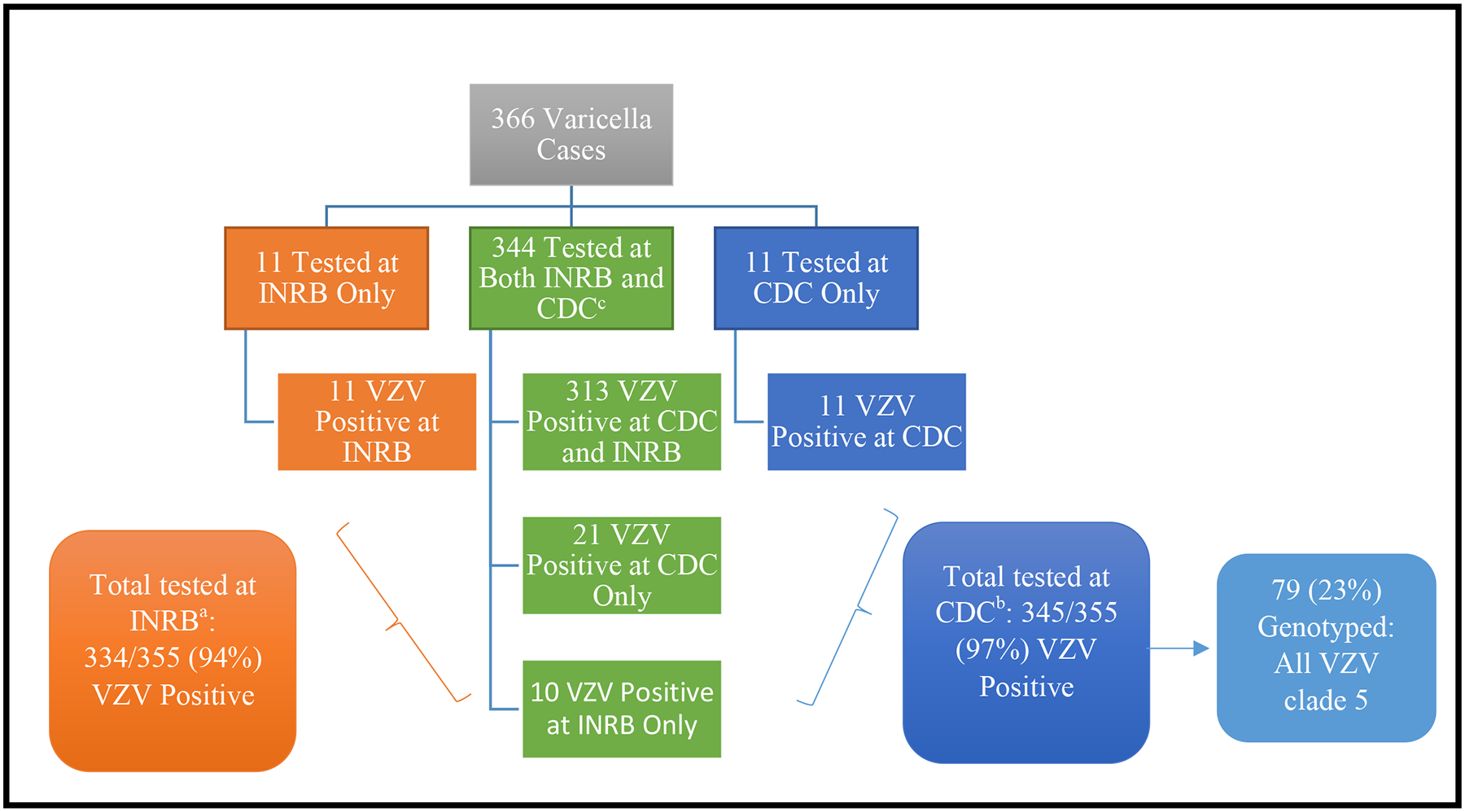
Methods: Demographic, clinical and epidemiological data were collected from each suspected monkeypox case 2009-2014. Samples were tested by PCR for both Orthopoxviruses and varicella-zoster virus (VZV); a subset of VZV-positive samples was genotyped. We defined a varicella case as a rash illness with laboratory-confirmed VZV.
Results: There were 366 varicella cases were identified; 66% were ≤19 years old. Most patients had non-typical varicella rash with lesions reported as the same size and stage of evolution (86%), deep and profound (91%), on palms of hands and/or soles of feet (86%) and not itchy (49%). Many had non-typical signs and symptoms, such as lymphadenopathy (70%) and sensitivity to light (23%). A higher proportion of persons aged ≥20 years than persons aged ≤19 years had ≥50 lesions (79% vs. 65%, P = 0.007) and were bedridden (15% vs. 9%, P = 0.056). All VZV isolates genotyped from 79 varicella cases were clade 5. During the surveillance period, one possible VZV-related death occurred in a 7-year-old child.
Conclusions: A large proportion of patients presented with non-typical varicella rash and clinical signs and symptoms, highlighting challenges identifying varicella in an area with endemic monkeypox. Continued surveillance and laboratory diagnosis will help in rapid identification and control of both monkeypox and varicella and improve our understanding of varicella epidemiology in Africa.
Objectif: Décrire les cas de varicelle identifiés dans la province de Tshuapa en République Démocratique du Congo (RDC) au cours de la surveillance de la variole du singe (monkeypox). MÉTHODES: Des données démographiques, cliniques et épidémiologiques ont été recueillies pour chaque cas présumé de monkeypox entre 2009 et 2014. Les échantillons ont été testés par PCR pour les orthopoxvirus et le virus varicelle-zona (VZV); un sous-ensemble d’échantillons positifs au VZV a été génotypé. Nous avons défini un cas de varicelle comme une éruption cutanée avec confirmation du VZV en laboratoire. RÉSULTATS: 366 cas de varicelle ont été identifiés; 66% avaient 19 ans ou moins. La plupart des patients présentaient une éruption non typique de varicelle avec des lésions rapportées de la même taille et le même stade d’évolution (86%), profonds (91%), sur la paume des mains et/ou la plante des pieds (86%), sans démangeaisons (49%). Nombre d'entre eux présentaient des signes et des symptômes inhabituels, tels qu'une adénopathie lymphatique (70%) et une sensibilité à la lumière (23%). Une proportion plus élevée de personnes âgées de 20 ans et plus que de personnes âgées de 19 ans et moins avaient 50 lésions ou plus (79% contre 65%, p = 0,007) et étaient alitées (15% contre 9%; p = 0,056). Tous les isolats de VZV génotypés chez 79 cas de varicelle appartenaient au clade 5. Au cours de la période de surveillance, un décès possible lié au VZV est survenu chez un enfant de 7 ans.
Conclusions: Une forte proportion de patients ont présenté une éruption de varicelle ainsi que des signes et symptômes cliniques non typiques, soulignant les difficultés rencontrées pour identifier la varicelle dans une zone endémique pour le monkeypox. Une surveillance continue et des diagnostics de laboratoire aideront à identifier et à contrôler rapidement le monkeypox et la varicelle et à améliorer notre compréhension sur l’épidémiologie de la varicelle en Afrique.
Keywords: RDC; Africa; Afrique; Democratic Republic of Congo, DRC; République Démocratique du Congo; chickenpox; epidemiology; monkeypox; varicella; varicella-zoster virus; varicelle; variole du singe monkeypox; virus varicelle-zona; Épidémiologie.
© 2019 John Wiley & Sons Ltd This article has been contributed to by US Government employees and their work is in the public domain in the USA.
Conflict of interest statement
Conflicts of interest:
None
Figures

References
-
- Seward JF, Marin M; On bahlf of the VZV Sage Working Group. Varicella Disease Burden and Varicella Vaccines. Available at: https://www.scribd.com/document/365929945/2-SAGE-April-VZV-Seward-Varicella. Accessed 12 April 2018.
-
- Gershon A, Takahashi M, and Seward JF, Varicella vaccine, in Vaccines, Plotkin S, Orenstein W, and Offit P, Editors. 2008, Saunders Elsevier. p. 915–958.
-
- WHO. World Health Organization, SAGE working group on varicella and herpes zoster vaccines. Background paper on varicella vaccine. Available at http://www.who.int/immunization/sage/meetings/2014/april/1_SAGE_varicell..., last accessed April 20, 2016. 2014.
-
- Spoulou V, et al., Implementing Universal Varicella Vaccination in Europe: The Path Forward. Pediatr Infect Dis J, 2018. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
