

Force of Infection and True Infection Rate of Dengue in Singapore: Implications for Dengue Control and Management
- PMID: 31062837
- PMCID: PMC6670050
- DOI: 10.1093/aje/kwz110
Force of Infection and True Infection Rate of Dengue in Singapore: Implications for Dengue Control and Management
Abstract
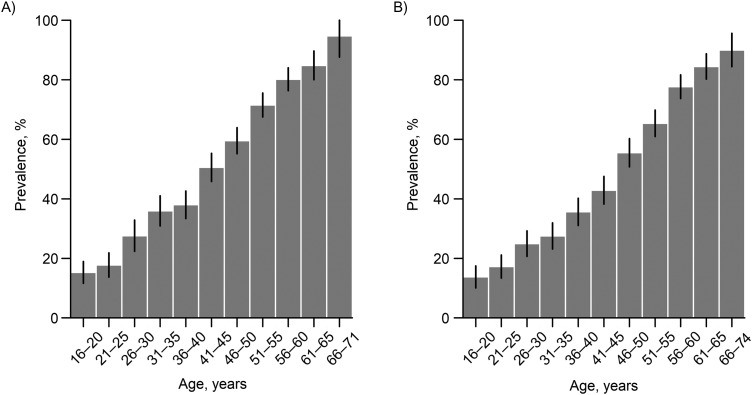
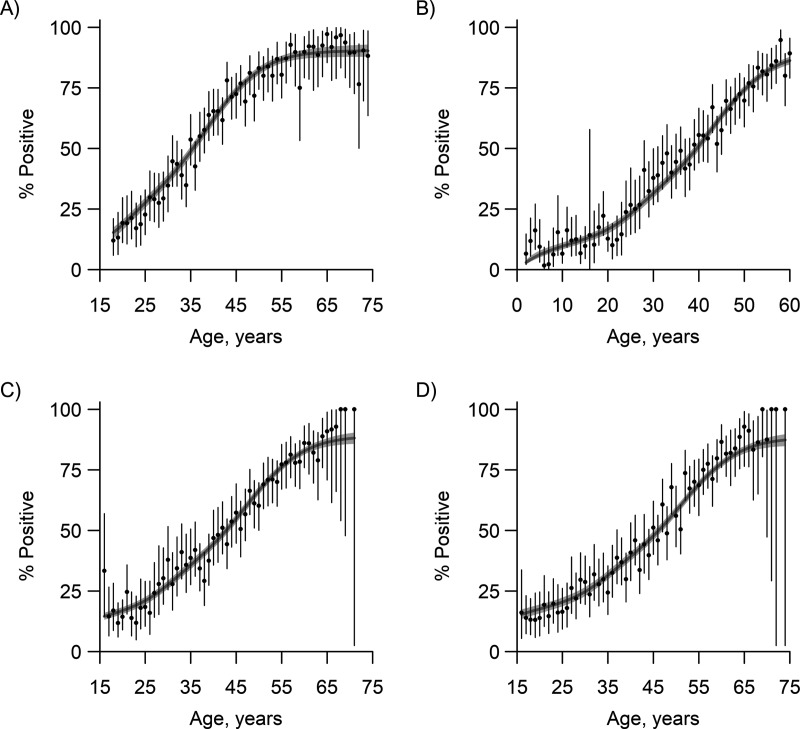
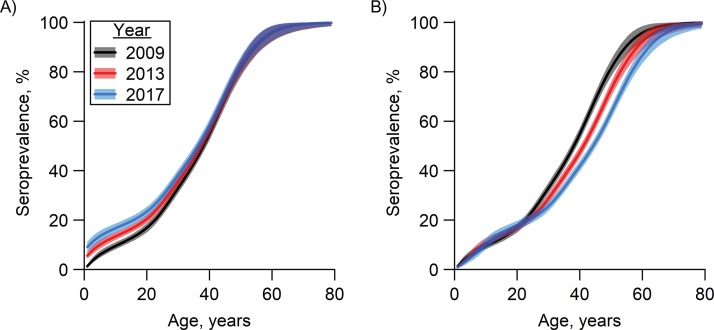
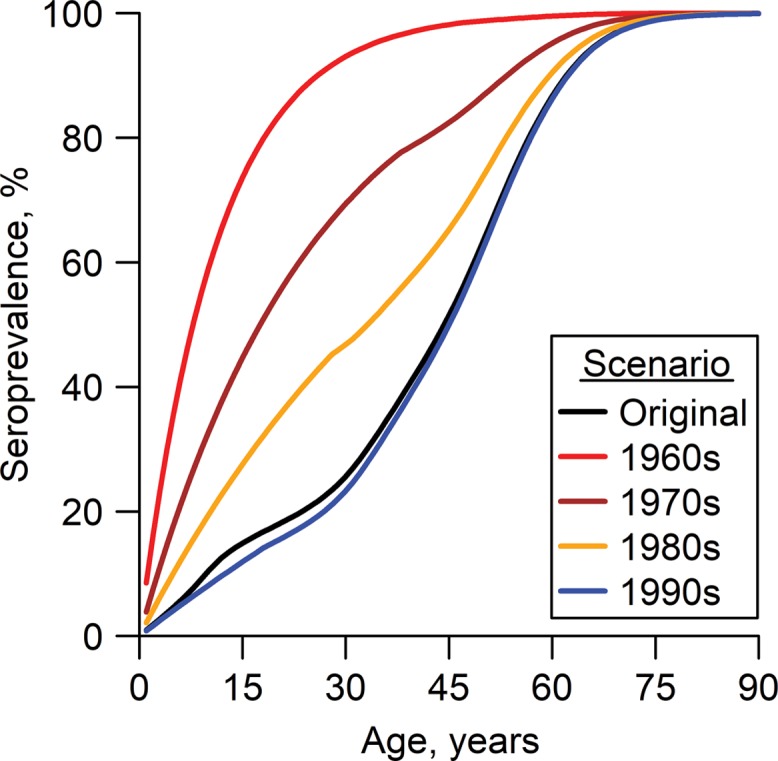
National data on dengue notifications do not capture all dengue infections and do not reflect the true intensity of disease transmission. To assess the true dengue infection rate and disease control efforts in Singapore, we conducted age-stratified serosurveys among residents after a 2013 outbreak that was the largest dengue outbreak on record. The age-weighted prevalence of dengue immunoglobulin G among residents was 49.8% (95% confidence interval: 48.4, 51.1) in 2013 and 48.6% (95% confidence interval: 47.0, 50.0) in 2017; prevalence increased with age. Combining these data with those from previous serosurveys, the year-on-year estimates of the dengue force of infection from 1930 to 2017 revealed a significant decrease from the late 1960s to the mid-1990s, after which the force of infection remained stable at approximately 10 per 1,000 persons per year. The reproduction number (R0) had also declined since the 1960s. The reduction in dengue transmission may be attributed to the sustained national vector program and partly to a change in the age structure of the population. The improved estimated ratio of notified cases to true infections, from 1:14 in 2005-2009 to 1:6 in 2014-2017, signifies that the national notification system, which relies on diagnosed cases, has improved over time. The data also suggest that the magnitudes of dengue epidemics cannot be fairly compared across calendar years and that the current disease control program remains applicable.
Keywords: Bayesian model; basic reproduction number; dengue; force of infection; infectious disease; seroprevalence; vector control.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health.
Figures


References
-
- World Health Organization Dengue and severe dengue. (Fact sheet no. 117). 2017. http://www.who.int/mediacentre/factsheets/fs117/en/. Accessed October 30, 2017.
-
- World Health Organization Global Strategy for Dengue Prevention and Control, 2012–2020 Geneva, Switzerland: World Health Organization; 2012. http://www.who.int/denguecontrol/9789241504034/en. Accessed October 30, 2017.
-
- Suaya JA, Shepard DS, Beatty ME Dengue: burden of disease and costs of illness. (Working paper 32). In: Report of the Scientific Working Group on Dengue, Geneva, 1–5 October 2006 Geneva, Switzerland: World Health Organization; 2007:35–49.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
