

Modelling diverse sources of Clostridium difficile in the community: importance of animals, infants and asymptomatic carriers
- PMID: 31063089
- PMCID: PMC6518831
- DOI: 10.1017/S0950268819000384
Modelling diverse sources of Clostridium difficile in the community: importance of animals, infants and asymptomatic carriers
Abstract
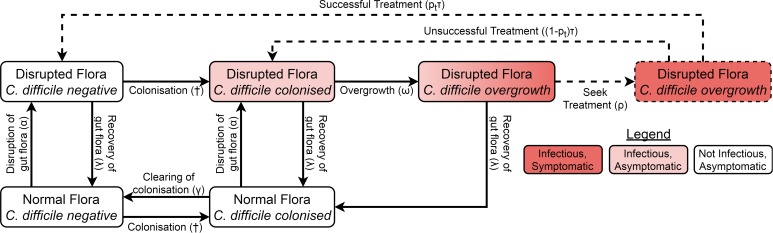
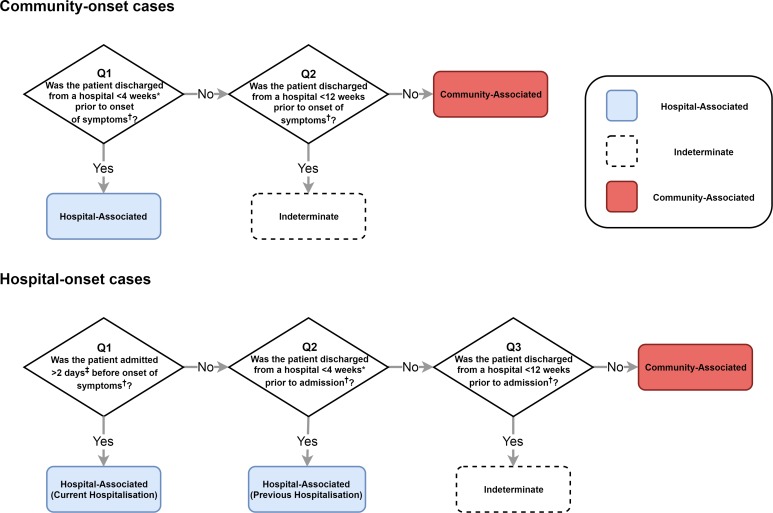
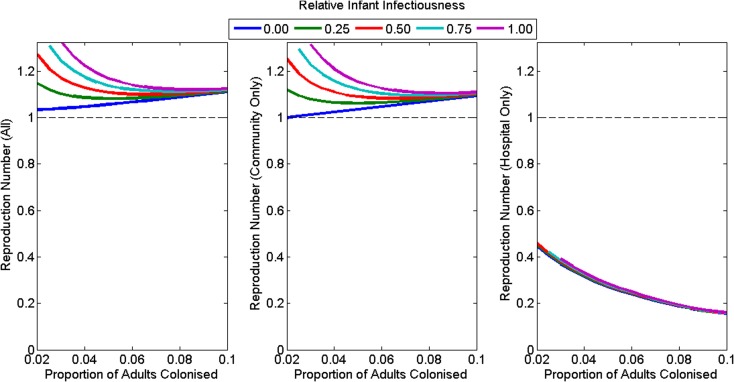
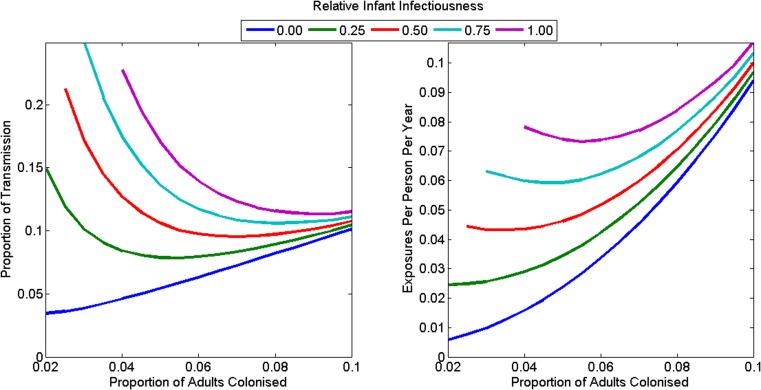
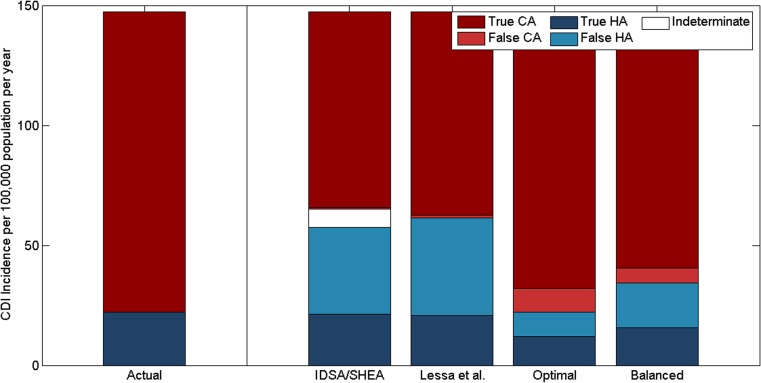
Clostridium difficile infections (CDIs) affect patients in hospitals and in the community, but the relative importance of transmission in each setting is unknown. We developed a mathematical model of C. difficile transmission in a hospital and surrounding community that included infants, adults and transmission from animal reservoirs. We assessed the role of these transmission routes in maintaining disease and evaluated the recommended classification system for hospital- and community-acquired CDIs. The reproduction number in the hospital was 1 for nearly all scenarios without transmission from animal reservoirs (range: 1.0-1.34). However, the reproduction number for the human population was 3.5-26.0%) of human exposures originated from animal reservoirs. Symptomatic adults accounted for <10% transmission in the community. Under conservative assumptions, infants accounted for 17% of community transmission. An estimated 33-40% of community-acquired cases were reported but 28-39% of these reported cases were misclassified as hospital-acquired by recommended definitions. Transmission could be plausibly sustained by asymptomatically colonised adults and infants in the community or exposure to animal reservoirs, but not hospital transmission alone. Under-reporting of community-onset cases and systematic misclassification underplays the role of community transmission.
Keywords: Clostridium difficile; community-acquired infection; hospital-acquired infection; mathematical disease model; zoonotic infection.
Conflict of interest statement
None.
Figures
Similar articles
-
Diverse Sources and Latent Reservoirs of Community-Associated Clostridioides difficile Infection.Clin Infect Dis. 2025 Feb 5;80(1):37-42. doi: 10.1093/cid/ciae429. Clin Infect Dis. 2025. PMID: 39215602 Review.
-
New insights into transmission of Clostridium difficile infection-narrative review.Clin Microbiol Infect. 2018 May;24(5):483-492. doi: 10.1016/j.cmi.2018.01.027. Epub 2018 Feb 7. Clin Microbiol Infect. 2018. PMID: 29427800 Review.
-
Clostridium difficile classification overestimates hospital-acquired infections.J Hosp Infect. 2018 Aug;99(4):453-460. doi: 10.1016/j.jhin.2017.12.014. Epub 2017 Dec 16. J Hosp Infect. 2018. PMID: 29258917
-
Healthcare-Associated Clostridium difficile Infections are Sustained by Disease from the Community.Bull Math Biol. 2017 Oct;79(10):2242-2257. doi: 10.1007/s11538-017-0328-8. Epub 2017 Aug 3. Bull Math Biol. 2017. PMID: 28776206
-
Clostridium difficile and One Health.Clin Microbiol Infect. 2020 Jul;26(7):857-863. doi: 10.1016/j.cmi.2019.10.023. Epub 2019 Nov 1. Clin Microbiol Infect. 2020. PMID: 31682985 Review.
Cited by
-
Clostridioides difficile phage biology and application.FEMS Microbiol Rev. 2021 Sep 8;45(5):fuab012. doi: 10.1093/femsre/fuab012. FEMS Microbiol Rev. 2021. PMID: 33580957 Free PMC article. Review.
-
Mucosal Vaccination Strategies against Clostridioides difficile Infection.Vaccines (Basel). 2023 Apr 23;11(5):887. doi: 10.3390/vaccines11050887. Vaccines (Basel). 2023. PMID: 37242991 Free PMC article. Review.
-
High Prevalence of Multidrug-Resistant Clostridioides difficile Following Extensive Use of Antimicrobials in Hospitalized Patients in Kenya.Front Cell Infect Microbiol. 2021 Feb 8;10:604986. doi: 10.3389/fcimb.2020.604986. eCollection 2020. Front Cell Infect Microbiol. 2021. PMID: 33628744 Free PMC article.
-
The contribution of community transmission to the burden of hospital-associated pathogens: A systematic scoping review of epidemiological models.One Health. 2024 Dec 16;20:100951. doi: 10.1016/j.onehlt.2024.100951. eCollection 2025 Jun. One Health. 2024. PMID: 39816238 Free PMC article. Review.
-
Some simple rules for estimating reproduction numbers in the presence of reservoir exposure or imported cases.Theor Popul Biol. 2020 Aug;134:182-194. doi: 10.1016/j.tpb.2020.04.002. Epub 2020 Apr 15. Theor Popul Biol. 2020. PMID: 32304644 Free PMC article.
References
-
- Jarvis WR et al. (2009) National point prevalence of Clostridium difficile in US health care facility inpatients, 2008. American Journal of Infection Control 37, 263–270. - PubMed
-
- Slimings C et al. (2014) Increasing incidence of Clostridium difficile infection, Australia, 2011–2012. The Medical Journal of Australia 200, 272–276. - PubMed
-
- Scallan E et al. (2006) Factors associated with seeking medical care and submitting a stool sample in estimating the burden of foodborne illness. Foodborne Pathogens and Disease 3, 432–438. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
