

Artificial intelligence at the intersection of pathology and radiology in prostate cancer
- PMID: 31063138
- PMCID: PMC6521904
- DOI: 10.5152/dir.2019.19125
Artificial intelligence at the intersection of pathology and radiology in prostate cancer
Abstract
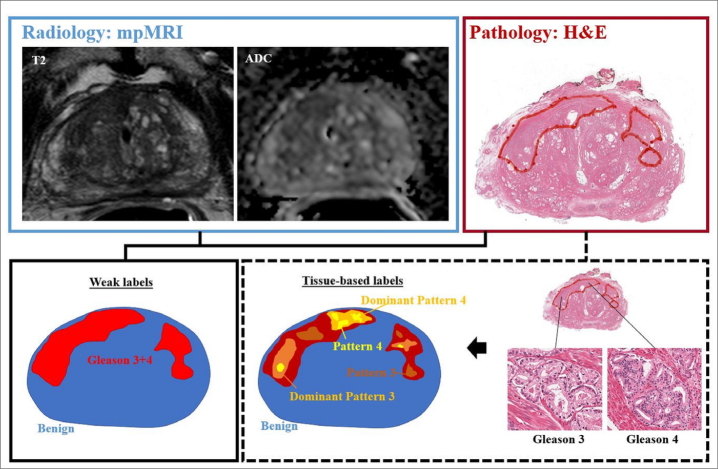
Pathologic grading plays a key role in prostate cancer risk stratification and treatment selection, traditionally assessed from systemic core needle biopsies sampled throughout the prostate gland. Multiparametric magnetic resonance imaging (mpMRI) has become a well-established clinical tool for detecting and localizing prostate cancer. However, both pathologic and radiologic assessment suffer from poor reproducibility among readers. Artificial intelligence (AI) methods show promise in aiding the detection and assessment of imaging-based tasks, dependent on the curation of high-quality training sets. This review provides an overview of recent advances in AI applied to mpMRI and digital pathology in prostate cancer which enable advanced characterization of disease through combined radiology-pathology assessment.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- Gleason DF. Classification of prostatic carcinomas. Cancer Chemother Rep. 1966;50:125–128. - PubMed
-
- Epstein JI, Egevad L, Amin MB, et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am J Surg Pathol. 2016;40:244–252. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
