

Oncolytic HSV therapy increases trametinib access to brain tumors and sensitizes them in vivo
- PMID: 31063549
- PMCID: PMC7571492
- DOI: 10.1093/neuonc/noz079
Oncolytic HSV therapy increases trametinib access to brain tumors and sensitizes them in vivo
Abstract
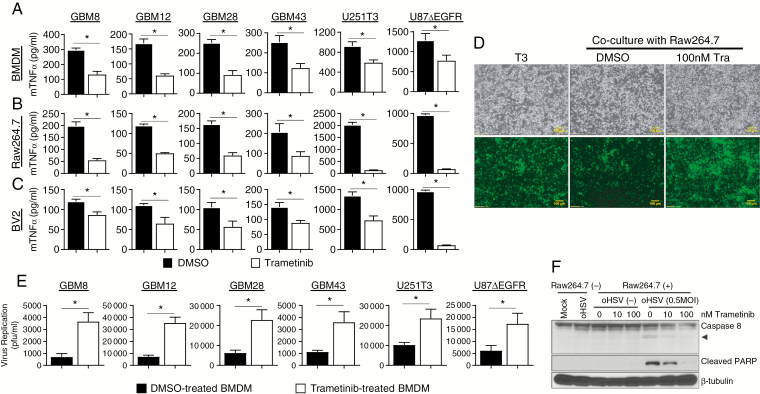
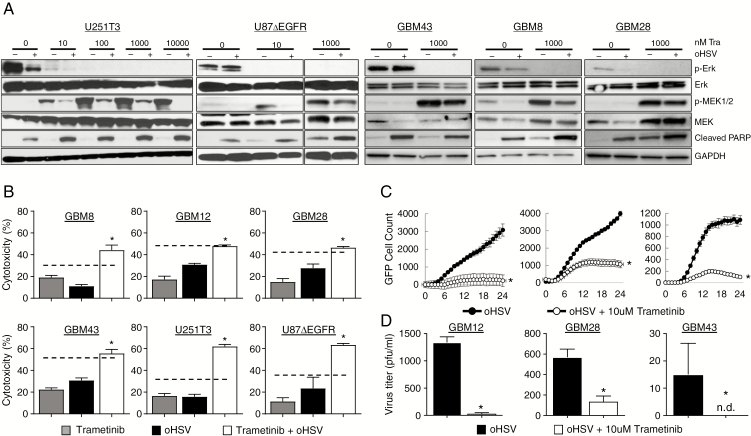
Background: Hyperactivation of the RAS-RAF-MEK-ERK signaling pathway is exploited by glioma cells to promote their growth and evade apoptosis. MEK activation in tumor cells can increase replication of ICP34.5-deleted herpes simplex virus type 1 (HSV-1), but paradoxically its activation in tumor-associated macrophages promotes a pro-inflammatory signaling that can inhibit virus replication and propagation. Here we investigated the effect of blocking MEK signaling in conjunction with oncolytic HSV-1 (oHSV) for brain tumors.
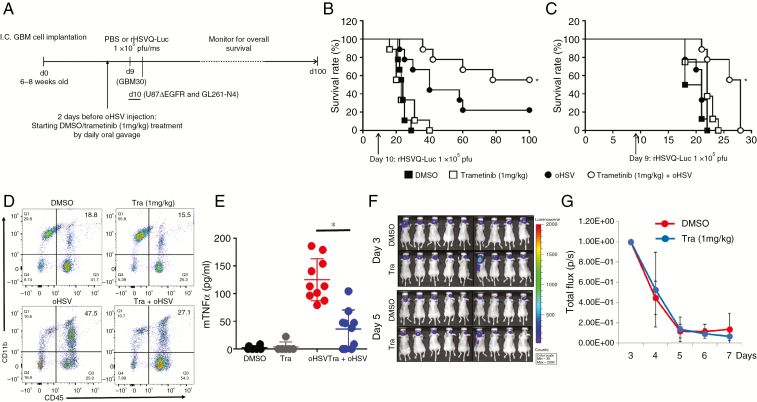
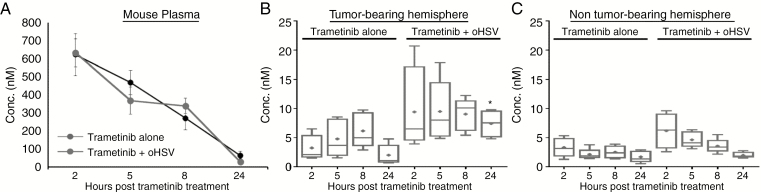
Methods: Infected glioma cells co-cultured with microglia or macrophages treated with or without trametinib were used to test trametinib effect on macrophages/microglia. Enzyme-linked immunosorbent assay, western blotting, and flow cytometry were utilized to evaluate the effect of the combination therapy. Pharmacokinetic (PK) analysis of mouse plasma and brain tissue was used to evaluate trametinib delivery to the CNS. Intracranial human and mouse glioma-bearing immune deficient and immune competent mice were used to evaluate the antitumor efficacy.
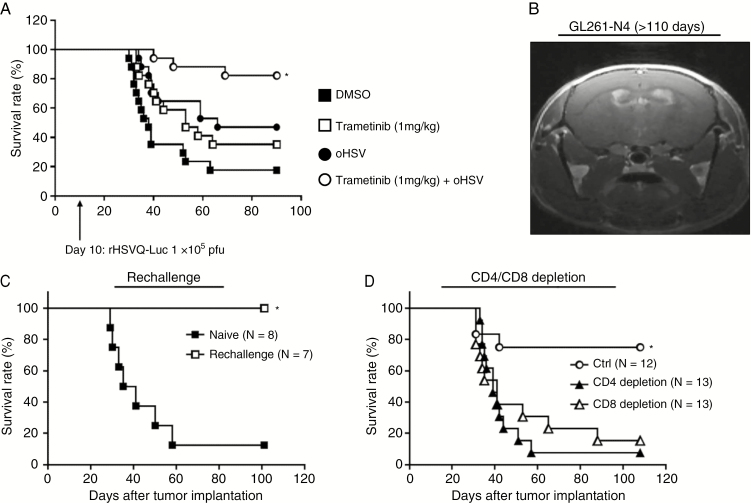
Result: Oncolytic HSV treatment rescued trametinib-mediated feedback reactivation of the mitogen-activated protein kinase signaling pathway in glioma. In vivo, PK analysis revealed enhanced blood-brain barrier penetration of trametinib after oHSV treatment. Treatment by trametinib, a MEK kinase inhibitor, led to a significant reduction in microglia- and macrophage-derived tumor necrosis factor alpha (TNFα) secretion in response to oHSV treatment and increased survival of glioma-bearing mice. Despite the reduced TNFα production observed in vivo, the combination treatment activated CD8+ T-cell mediated immunity and increased survival in a glioma-bearing immune-competent mouse model.
Conclusion: This study provides a rationale for combining oHSV with trametinib for the treatment of brain tumors.
Keywords: RAS-RAF-MEK-ERK signaling; glioblastoma (GBM); oncolytic herpes simplex virus-1 (oHSV); trametinib; tumor necrosis factor α (TNFα).
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Antitumor immune response during glioma virotherapy.Neuro Oncol. 2019 Sep 6;21(9):1087-1088. doi: 10.1093/neuonc/noz114. Neuro Oncol. 2019. PMID: 31348516 Free PMC article. No abstract available.
References
-
- Jo J, Wen PY. Antiangiogenic therapy of high-grade gliomas. Prog Neurol Surg. 2018;31:180–199. - PubMed
-
- Long GV, Stroyakovskiy D, Gogas H, et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet. 2015;386(9992):444–451. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
