

The effect of adhesive tape versus endotracheal tube fastener in critically ill adults: the endotracheal tube securement (ETTS) randomized controlled trial
- PMID: 31064406
- PMCID: PMC6505126
- DOI: 10.1186/s13054-019-2440-7
The effect of adhesive tape versus endotracheal tube fastener in critically ill adults: the endotracheal tube securement (ETTS) randomized controlled trial
Abstract
Background: The optimal securement method of endotracheal tubes is unknown but should prevent dislodgement while minimizing complications. The use of an endotracheal tube fastener might reduce complications among critically ill adults undergoing endotracheal intubation.
Methods: In this pragmatic, single-center, randomized trial, critically ill adults admitted to the medical intensive care unit (MICU) and expected to require invasive mechanical ventilation for greater than 24 h were randomized to adhesive tape or endotracheal tube fastener at the time of intubation. The primary endpoint was a composite of any of the following: presence of lip ulcer, endotracheal tube dislodgement (defined as moving at least 2 cm), ventilator-associated pneumonia, or facial skin tears anytime between randomization and the earlier of death or 48 h after extubation. Secondary endpoints included duration of mechanical ventilation and ICU and in-hospital mortality.
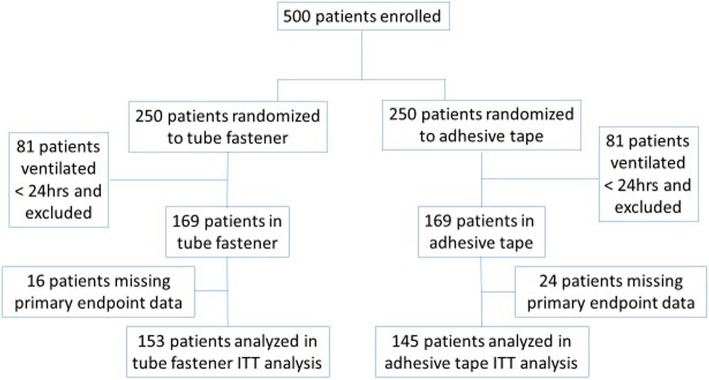
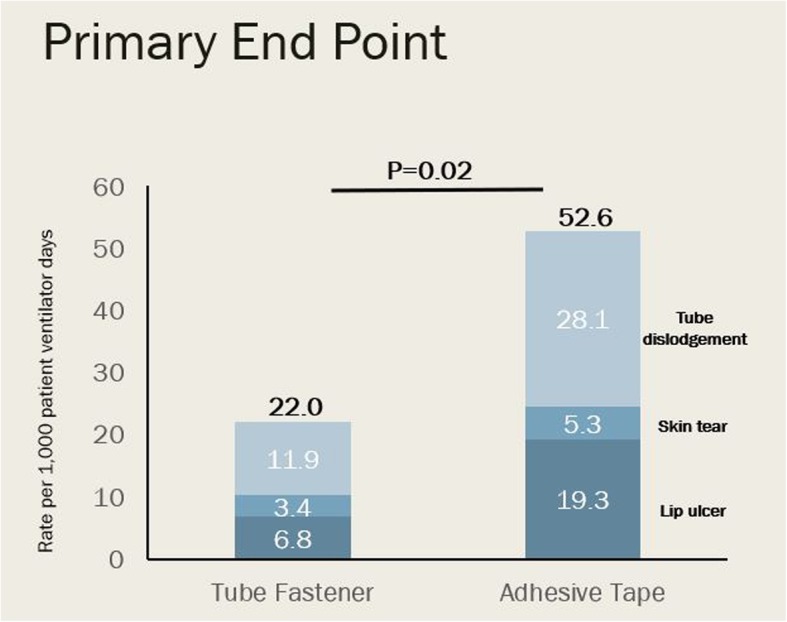
Results: Of 500 patients randomized over a 12-month period, 162 had a duration of mechanical ventilation less than 24 h and 40 had missing outcome data, leaving 153 evaluable patients randomized to tube fastener and 145 evaluable patients randomized to adhesive tape. Baseline characteristics were similar between the groups. The primary endpoint occurred 13 times in 12 (7.8%) patients in the tube fastener group and 30 times in 25 (17.2%) patients in the adhesive tape group (p = 0.014) for an overall incidence of 22.0 versus 52.6 per 1000 ventilator days, respectively (p = 0.020). Lip ulcers occurred in 4 (2.6%) versus 11 (7.3%) patients, or an incidence rate of 6.5 versus 19.5 per 1000 patient ventilator days (p = 0.053) in the fastener and tape groups, respectively. The endotracheal tube was dislodged 7 times in 6 (3.9%) patients in the tube fastener group and 16 times in 15 (10.3%) patients in the tape group (p = 0.03), reflecting incidences of 11.9 and 28.1 per 1000 ventilator days, respectively. Facial skin tears were similar between the groups. Mechanical ventilation duration and ICU and hospital mortality did not differ.
Conclusion: The use of the endotracheal tube fastener to secure the endotracheal tubes reduces the rate of a composite outcome that included lip ulcers, facial skin tears, or endotracheal tube dislodgement compared to adhesive tape.
Trial registration: ClinicalTrials.gov NCT03760510. Retrospectively registered on November 30, 2018.
Keywords: Critical care; Endotracheal tube; Endotracheal tube dislodgement; Facial skin tear; Intensive care units; Lip ulcer; Mechanical ventilation; Tube fastener.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol has been reviewed by the Institutional Review Board (IRB) Health Science Committee 1 at Vanderbilt University, and the need for informed consent from the patients was waived with a participant notification sheet (#170596).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mohammad H, Hassan M. Endotracheal tube securements: effectiveness of three techniques among orally intubated patients. Egyptian J Chest Dis Tuberc. 2015;64:183–196. doi: 10.1016/j.ejcdt.2014.09.006. - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
