

Cost-Effectiveness of the Use of Autologous Cell Harvesting Device Compared to Standard of Care for Treatment of Severe Burns in the United States
- PMID: 31065995
- PMCID: PMC6647544
- DOI: 10.1007/s12325-019-00961-2
Cost-Effectiveness of the Use of Autologous Cell Harvesting Device Compared to Standard of Care for Treatment of Severe Burns in the United States
Abstract
Introduction: When introducing a new intervention into burn care, it is important to consider both clinical and economic impacts, as the financial burden of burns in the USA is significant. This study utilizes a health economic modeling approach to estimate cost-effectiveness and burn center budget-impact for the use of the RECELL® Autologous Cell Harvesting Device to prepare autologous skin cell suspension (ASCS) compared to standard of care (SOC) split-thickness skin graft (STSG) for the treatment of severe burn injuries requiring surgical intervention for definitive closure.
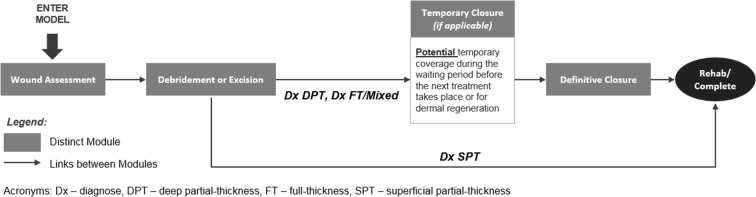
Methods: A hospital-perspective model using sequential decision trees depicts the acute burn care pathway (wound assessment, debridement/excision, temporary coverage, definitive closure) and predicts the relative differences between use of ASCS compared to SOC. Clinical inputs and ASCS impact on length of stay (LOS) were derived from clinical trials and real-world use data, American Burn Association National Burn Repository database analyses, and burn surgeon interviews. Hospital resource use and unit costs were derived from three US burn centers. A budget impact calculation leverages Monte Carlo simulation to estimate the overall impact to a burn center.
Results: ASCS treatment is cost-saving or cost-neutral (< 2% difference) and results in lower LOS compared to SOC across expected patient profiles and scenarios. In aggregate, ASCS treatment saves a burn center 14-17.3% annually. Results are sensitive to, but remain robust across, changing assumptions for relative impact of ASCS use on LOS, procedure time, and number of procedures.
Conclusions: Use of ASCS compared to SOC reduces hospital costs and LOS of severe burns in the USA.
Funding: AVITA Medical.
Keywords: Autologous cell harvesting device; Budget impact; Burn care; Cost-effectiveness; Dermatology; Skin graft; Split-thickness.
Figures
References
-
- Pruitt B, Mason A. Epidemiological, demographic, and outcome characteristics of burn injury. In: Herndon D, editor. Total burn care. London: Saunders; 1996. p. 13.
-
- American Burn Association. Burn incidence and treatment in the United States: 2016. 2016. http://www.ameriburn.org/resources_factsheet.php. Accessed 3 Dec 2018.
-
- CDC. 20 Leading causes of nonfatal injury, United States. 2015, All races, both sexes, disposition: all cases. 2015. https://webappa.cdc.gov/sasweb/ncipc/nfilead.html. Accessed 5 Mar 2018.
-
- National Institutes of Health. Research portfolio online reporting tools. Burns and traumatic injury 2010. 2010. https://report.nih.gov/nihfactsheets/Pdfs/BurnsandTraumaticInjury(NIGMS).... Accessed 6 Apr 2017.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
