

Prospective Clinical and Molecular Evaluation of Potential Plasmodium ovale curtisi and wallikeri Relapses in a High-transmission Setting
- PMID: 31066448
- PMCID: PMC6880329
- DOI: 10.1093/cid/ciz131
Prospective Clinical and Molecular Evaluation of Potential Plasmodium ovale curtisi and wallikeri Relapses in a High-transmission Setting
Abstract
Background: Plasmodium ovale curtisi and wallikeri are perceived as relapsing malarial parasites. Contrary to Plasmodium vivax, direct evidence for this hypothesis is scarce. The aim of this prospective study was to characterize the reappearance patterns of ovale parasites.
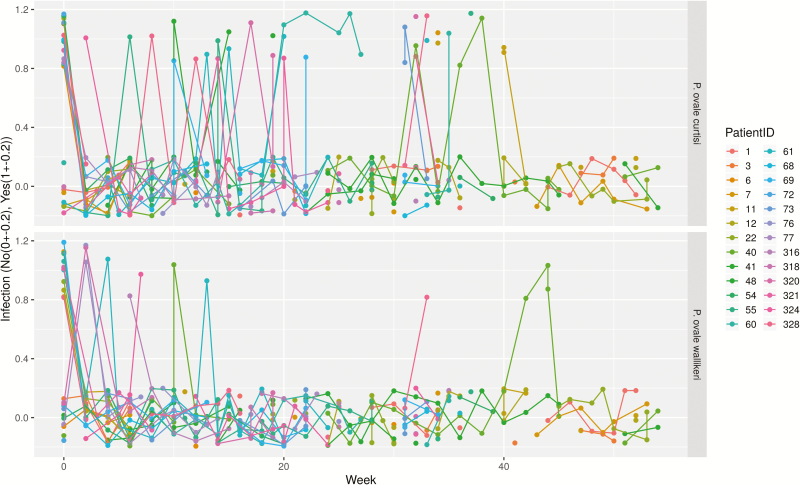
Methods: P. ovale spp. infected patients were treated with artemether-lumefantrine and followed biweekly for up to 1 year for the detection of reappearing parasitemia. Molecular analysis of reappearing isolates was performed to identify homologous isolates by genotyping and to define cases of relapse following predefined criteria.
Results: At inclusion, 26 participants were positive for P. ovale curtisi and/or P. ovale wallikeri. The median duration of follow-up was 35 weeks. Reappearance of the same P. ovale species was observed in 46% of participants; 61% of P. ovale curtisi and 19% of P. ovale wallikeri infection-free intervals were estimated to end with reappearance by week 32. Based on the predefined criteria, 23% of participants were identified with 1 or 2 relapses, all induced by P. ovale curtisi.
Conclusion: These findings are in line with the currently accepted relapse theory inasmuch as the reappearance of P. ovale curtisi strains following initial blood clearance was conclusively demonstrated. Interestingly, no relapse of P. ovale wallikeri was observed.
Keywords: Plasmodium ovale; Plasmodium ovale curtisi; Plasmodium ovale wallikeri; CERMEL; relapse.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures




Comment in
-
Non-falciparum Malaria in Africa and Learning From Plasmodium vivax in Asia.Clin Infect Dis. 2020 Apr 15;70(9):2018-2019. doi: 10.1093/cid/ciz780. Clin Infect Dis. 2020. PMID: 31408098 Free PMC article. No abstract available.
-
Reply to Lin et al.Clin Infect Dis. 2020 Apr 15;70(9):2019-2020. doi: 10.1093/cid/ciz781. Clin Infect Dis. 2020. PMID: 31408115 Free PMC article. No abstract available.
References
-
- Mueller I, Galinski MR, Baird JK, et al. . Key gaps in the knowledge of Plasmodium vivax, a neglected human malaria parasite. Lancet Infect Dis 2009; 9:555–66. - PubMed
-
- Stephens J. A new malaria parasite of man. Ann Trop Med Parasitol 1922; 16:383–6.
-
- Stephens J, Owen DU. Plasmodium ovale. Ann Trop Med Parasitol 1927; 21:293–302.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
