

Natural Language Processing for the Identification of Silent Brain Infarcts From Neuroimaging Reports
- PMID: 31066686
- PMCID: PMC6524454
- DOI: 10.2196/12109
Natural Language Processing for the Identification of Silent Brain Infarcts From Neuroimaging Reports
Abstract
Background: Silent brain infarction (SBI) is defined as the presence of 1 or more brain lesions, presumed to be because of vascular occlusion, found by neuroimaging (magnetic resonance imaging or computed tomography) in patients without clinical manifestations of stroke. It is more common than stroke and can be detected in 20% of healthy elderly people. Early detection of SBI may mitigate the risk of stroke by offering preventative treatment plans. Natural language processing (NLP) techniques offer an opportunity to systematically identify SBI cases from electronic health records (EHRs) by extracting, normalizing, and classifying SBI-related incidental findings interpreted by radiologists from neuroimaging reports.
Objective: This study aimed to develop NLP systems to determine individuals with incidentally discovered SBIs from neuroimaging reports at 2 sites: Mayo Clinic and Tufts Medical Center.
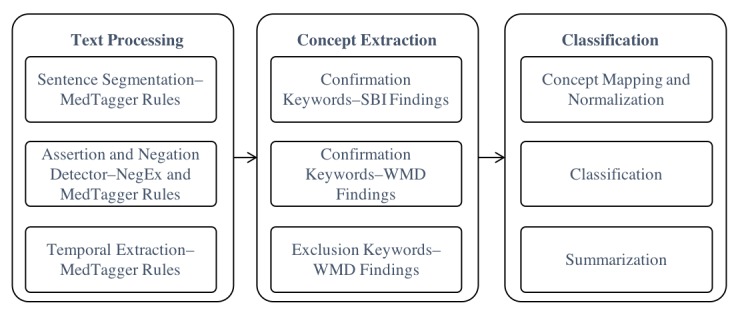
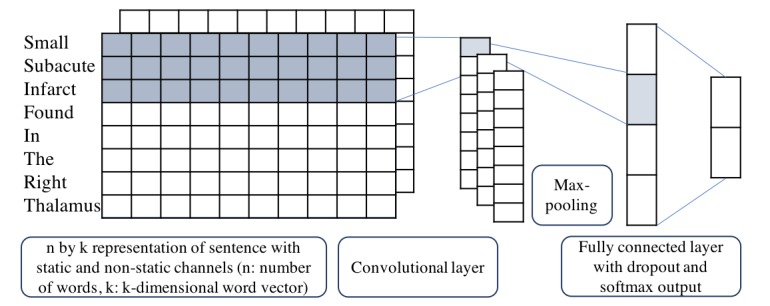
Methods: Both rule-based and machine learning approaches were adopted in developing the NLP system. The rule-based system was implemented using the open source NLP pipeline MedTagger, developed by Mayo Clinic. Features for rule-based systems, including significant words and patterns related to SBI, were generated using pointwise mutual information. The machine learning models adopted convolutional neural network (CNN), random forest, support vector machine, and logistic regression. The performance of the NLP algorithm was compared with a manually created gold standard. The gold standard dataset includes 1000 radiology reports randomly retrieved from the 2 study sites (Mayo and Tufts) corresponding to patients with no prior or current diagnosis of stroke or dementia. 400 out of the 1000 reports were randomly sampled and double read to determine interannotator agreements. The gold standard dataset was equally split to 3 subsets for training, developing, and testing.
Results: Among the 400 reports selected to determine interannotator agreement, 5 reports were removed due to invalid scan types. The interannotator agreements across Mayo and Tufts neuroimaging reports were 0.87 and 0.91, respectively. The rule-based system yielded the best performance of predicting SBI with an accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 0.991, 0.925, 1.000, 1.000, and 0.990, respectively. The CNN achieved the best score on predicting white matter disease (WMD) with an accuracy, sensitivity, specificity, PPV, and NPV of 0.994, 0.994, 0.994, 0.994, and 0.994, respectively.
Conclusions: We adopted a standardized data abstraction and modeling process to developed NLP techniques (rule-based and machine learning) to detect incidental SBIs and WMDs from annotated neuroimaging reports. Validation statistics suggested a high feasibility of detecting SBIs and WMDs from EHRs using NLP.
Keywords: electronic health records; natural language processing; neuroimaging.
©Sunyang Fu, Lester Y Leung, Yanshan Wang, Anne-Olivia Raulli, David F Kallmes, Kristin A Kinsman, Kristoff B Nelson, Michael S Clark, Patrick H Luetmer, Paul R Kingsbury, David M Kent, Hongfang Liu. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 21.04.2019.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Fanning J, Wong A, Fraser J. The epidemiology of silent brain infarction: a systematic review of population-based cohorts. BMC Med. 2014 Jul 9;12:119. doi: 10.1186/s12916-014-0119-0. https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-014-0119-0 s12916-014-0119-0 - DOI - PMC - PubMed
-
- Furie K, Kasner S, Adams R, Albers G, Bush R, Fagan S, Halperin JL, Johnston SC, Katzan I, Kernan WN, Mitchell PH, Ovbiagele B, Palesch YY, Sacco RL, Schwamm LH, Wassertheil-Smoller S, Turan TN, Wentworth D, American Heart Association Stroke Council‚ Council on Cardiovascular Nursing‚ Council on Clinical Cardiology‚Interdisciplinary Council on Quality of CareOutcomes Research Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2011 Jan;42(1):227–76. doi: 10.1161/STR.0b013e3181f7d043.STR.0b013e3181f7d043 - DOI - PubMed
-
- Gouw A, van der Flier WM, Fazekas F, van Straaten EC, Pantoni L, Poggesi A, Inzitari D, Erkinjuntti T, Wahlund LO, Waldemar G, Schmidt R, Scheltens P, Barkhof F, LADIS Study Group Progression of white matter hyperintensities and incidence of new lacunes over a 3-year period: the Leukoaraiosis and Disability study. Stroke. 2008 May;39(5):1414–20. doi: 10.1161/STROKEAHA.107.498535.STROKEAHA.107.498535 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
