

Individualized decision aid for diverse women with lupus nephritis (IDEA-WON): A randomized controlled trial
- PMID: 31067237
- PMCID: PMC6505936
- DOI: 10.1371/journal.pmed.1002800
Individualized decision aid for diverse women with lupus nephritis (IDEA-WON): A randomized controlled trial
Abstract
Background: Treatment decision-making regarding immunosuppressive therapy is challenging for individuals with lupus. We assessed the effectiveness of a decision aid for immunosuppressive therapy in lupus nephritis.
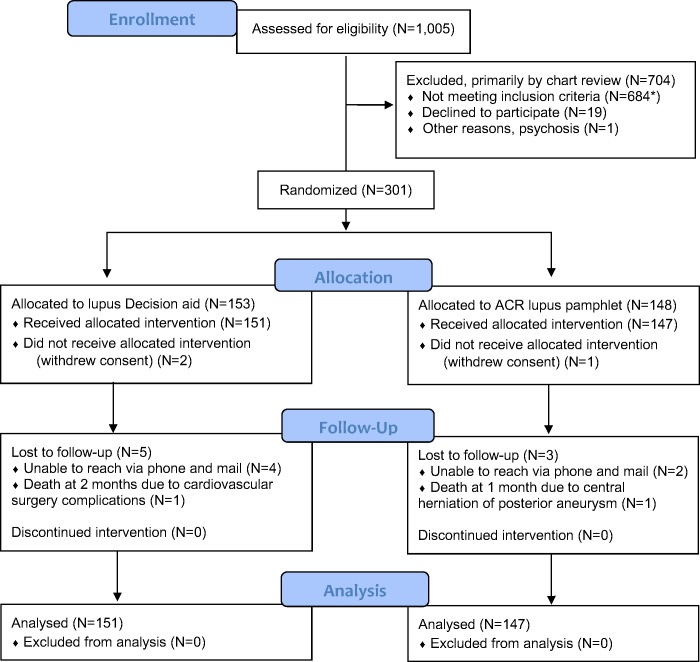
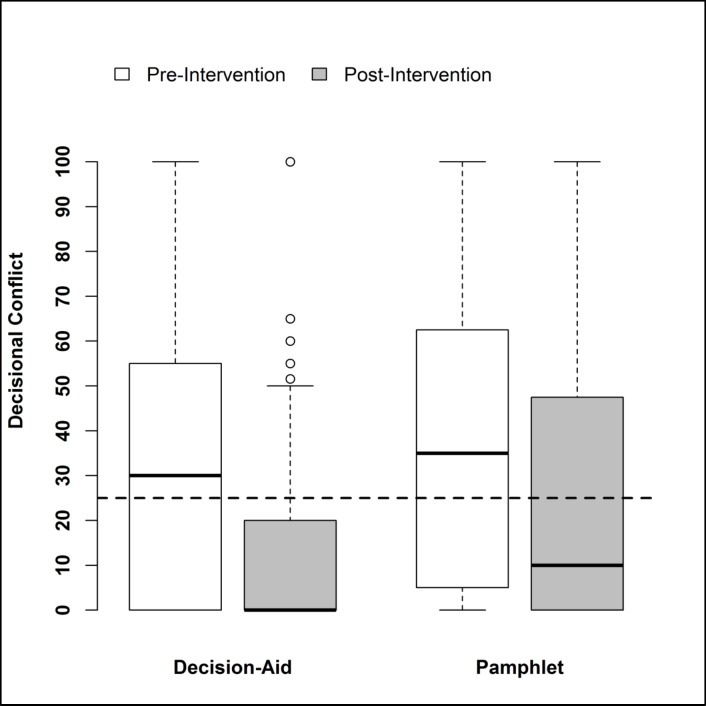
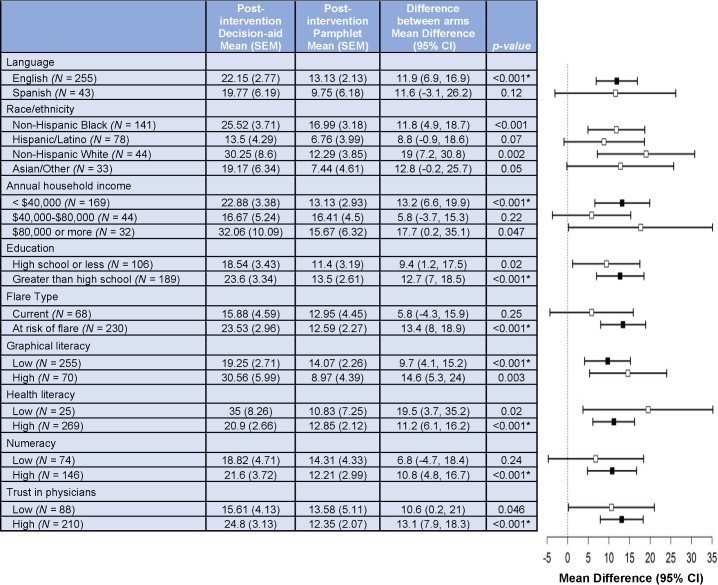
Methods and findings: In a United States multicenter, open-label, randomized controlled trial (RCT), adult women with lupus nephritis, mostly from racial/ethnic minority backgrounds with low socioeconomic status (SES), seen in in- or outpatient settings, were randomized to an individualized, culturally tailored, computerized decision aid versus American College of Rheumatology (ACR) lupus pamphlet (1:1 ratio), using computer-generated randomization. We hypothesized that the co-primary outcomes of decisional conflict and informed choice regarding immunosuppressive medications would improve more in the decision aid group. Of 301 randomized women, 298 were analyzed; 47% were African-American, 26% Hispanic, and 15% white. Mean age (standard deviation [SD]) was 37 (12) years, 57% had annual income of <$40,000, and 36% had a high school education or less. Compared with the provision of the ACR lupus pamphlet (n = 147), participants randomized to the decision aid (n = 151) had (1) a clinically meaningful and statistically significant reduction in decisional conflict, 21.8 (standard error [SE], 2.5) versus 12.7 (SE, 2.0; p = 0.005) and (2) no difference in informed choice in the main analysis, 41% versus 31% (p = 0.08), but clinically meaningful and statistically significant difference in sensitivity analysis (net values for immunosuppressives positive [in favor] versus negative [against]), 50% versus 35% (p = 0.006). Unresolved decisional conflict was lower in the decision aid versus pamphlet groups, 22% versus 44% (p < 0.001). Significantly more patients in the decision aid versus pamphlet group rated information to be excellent for understanding lupus nephritis (49% versus 33%), risk factors (43% versus 27%), medication options (50% versus 33%; p ≤ 0.003 for all); and the ease of use of materials was higher in the decision aid versus pamphlet groups (51% versus 38%; p = 0.006). Key study limitations were the exclusion of men, short follow-up, and the lack of clinical outcomes, including medication adherence.
Conclusions: An individualized decision aid was more effective than usual care in reducing decisional conflict for choice of immunosuppressive medications in women with lupus nephritis.
Trial registration: Clinicaltrials.gov, NCT02319525.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests. JAS has received research grants from Takeda and Savient Pharmaceuticals and consultant fees from Savient, Takeda, Regeneron, Merz, Iroko, Bioiberica, Crealta/Horizon, Fidia, and Allergan Pharmaceuticals and WebMD, UBM LLC, Medscape, and the American College of Rheumatology. JAS served as the principal investigator for an investigator-initiated study funded by Horizon Pharmaceuticals through a grant to DINORA, Inc., a 501 (c)(3) entity. JAS is a member of the executive of OMERACT, an organization that develops outcome measures in rheumatology, and receives arms-length funding from 36 companies; a member of the American College of Rheumatology's (ACR) Annual Meeting Planning Committee (AMPC); Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee; and a member of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and the Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis. MD serves on an Independent Data Monitoring Committee for Biogen, Genentech, and Janssen Pharmaceuticals and as a consultant to Abbvie, Kezar, and AstraZeneca. KLW reports grants and personal fees from Pfizer, grants and personal fees from BMS, personal fees from Abbvie, grants and personal fees from UCB, personal fees from Lilly, personal fees from Galapagos, and personal fees from GSK, outside the submitted work.
Figures

References
-
- Odutola J, Ward MM. Ethnic and socioeconomic disparities in health among patients with rheumatic disease. Current opinion in rheumatology. 2005;17(2):147–52. Epub 2005/02/16. . - PubMed
-
- Alarcon GS, Friedman AW, Straaton KV, Moulds JM, Lisse J, Bastian HM, et al. Systemic lupus erythematosus in three ethnic groups: III. A comparison of characteristics early in the natural history of the LUMINA cohort. LUpus in MInority populations: NAture vs. Nurture. Lupus. 1999;8(3):197–209. Epub 1999/05/26. 10.1191/096120399678847704 . - DOI - PubMed
-
- Krishnan E. Hospitalization and mortality of patients with systemic lupus erythematosus. The Journal of rheumatology. 2006;33(9):1770–4. Epub 2006/07/13. . - PubMed
