

EJE AWARD 2019: New diagnostic approaches for patients with polyuria polydipsia syndrome
- PMID: 31067508
- PMCID: PMC6598864
- DOI: 10.1530/EJE-19-0163
EJE AWARD 2019: New diagnostic approaches for patients with polyuria polydipsia syndrome
Abstract
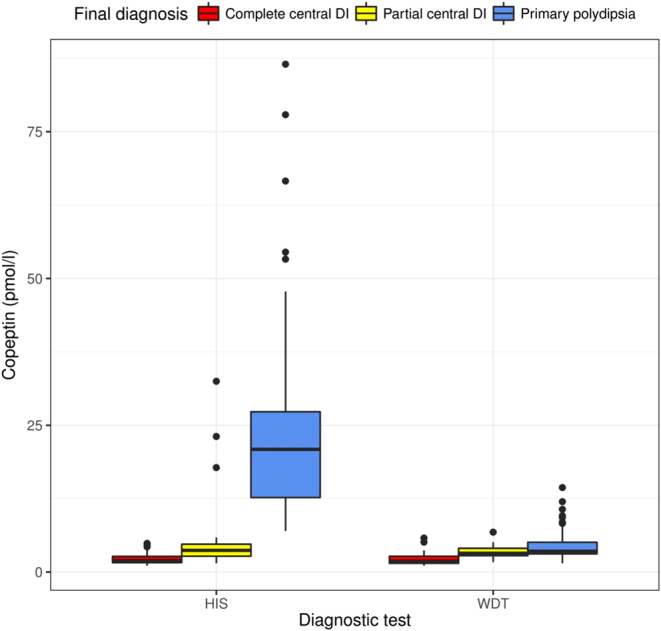
Diabetes insipidus (DI), be it from central or nephrogenic origin, must be differentiated from secondary forms of hypotonic polyuria such as primary polydipsia. Differentiation is crucial since wrong treatment can have deleterious consequences. Since decades, the gold standard for differentiation has been the water deprivation test, which has limitations leading to an overall unsatisfying diagnostic accuracy. Furthermore, it is cumbersome for patients with a long test duration. Clinical signs and symptoms and MRI characteristics overlap between patients with DI and primary polydipsia. The direct test including vasopressin (AVP) measurement upon osmotic stimulation was meant to overcome these limitations, but failed to enter clinical practice mainly due to technical constraints of the AVP assay. Copeptin is secreted in equimolar amount to AVP but can easily be measured with a sandwich immunoassay. A high correlation between copeptin and AVP has been shown. Accordingly, copeptin mirrors the amount of AVP in the circulation and has led to a 'revival' of the direct test in the differential diagnosis of DI. We have shown that a baseline copeptin, without prior thirsting, unequivocally identifies patients with nephrogenic DI. In contrast, for the differentiation between central DI and primary polydipsia, a stimulated copeptin level of 4.9 pmol/L upon hypertonic saline infusion differentiates these two entities with a high diagnostic accuracy and is superior to the water deprivation test. Close sodium monitoring during the test is a prerequisite. Further new test methods are currently evaluated and might provide an even simpler way of differential diagnosis in the future.
Figures




Similar articles
-
Comparative Diagnostic Performance of Copeptin After Hypertonic Saline Infusion Versus Water Deprivation Test in Pediatric Patients with Polyuria-Polydipsia Syndrome.Int J Mol Sci. 2025 Jun 6;26(12):5449. doi: 10.3390/ijms26125449. Int J Mol Sci. 2025. PMID: 40564913 Free PMC article.
-
Copeptin in the differential diagnosis of hypotonic polyuria.J Endocrinol Invest. 2020 Jan;43(1):21-30. doi: 10.1007/s40618-019-01087-6. Epub 2019 Jul 31. J Endocrinol Invest. 2020. PMID: 31368050 Review.
-
Diagnostic Accuracy of Copeptin in the Differential Diagnosis of the Polyuria-polydipsia Syndrome: A Prospective Multicenter Study.J Clin Endocrinol Metab. 2015 Jun;100(6):2268-74. doi: 10.1210/jc.2014-4507. Epub 2015 Mar 13. J Clin Endocrinol Metab. 2015. PMID: 25768671
-
Diabetes Insipidus: New Concepts for Diagnosis.Neuroendocrinology. 2020;110(9-10):859-867. doi: 10.1159/000505548. Epub 2020 Jan 2. Neuroendocrinology. 2020. PMID: 31986514 Review.
-
Arginine or Hypertonic Saline-Stimulated Copeptin to Diagnose AVP Deficiency.N Engl J Med. 2023 Nov 16;389(20):1877-1887. doi: 10.1056/NEJMoa2306263. N Engl J Med. 2023. PMID: 37966286 Clinical Trial.
Cited by
-
Transient severe hypotonic hyponatraemia in children - presentation of three cases.Pediatr Endocrinol Diabetes Metab. 2024;30(2):97-103. doi: 10.5114/pedm.2024.140933. Pediatr Endocrinol Diabetes Metab. 2024. PMID: 39026487 Free PMC article.
-
Everything in excess is opposed to nature, even vitamin D: a case report.Endocrinol Diabetes Metab Case Rep. 2022 Feb 1;2022:21-0181. doi: 10.1530/EDM-21-0181. Online ahead of print. Endocrinol Diabetes Metab Case Rep. 2022. PMID: 35170432 Free PMC article.
-
Psychogenic polydipsia in a female adolescent without a psychiatric background: A case report.Clin Case Rep. 2021 Feb 27;9(4):1937-1942. doi: 10.1002/ccr3.3910. eCollection 2021 Apr. Clin Case Rep. 2021. PMID: 33936619 Free PMC article.
-
Comparative Diagnostic Performance of Copeptin After Hypertonic Saline Infusion Versus Water Deprivation Test in Pediatric Patients with Polyuria-Polydipsia Syndrome.Int J Mol Sci. 2025 Jun 6;26(12):5449. doi: 10.3390/ijms26125449. Int J Mol Sci. 2025. PMID: 40564913 Free PMC article.
References
-
- Robertson GL. The regulation of vasopressin function in health and disease. Recent Progress in Hormone Research 1976. 33 . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
