

Veterans Affairs patient database (VAPD 2014-2017): building nationwide granular data for clinical discovery
- PMID: 31068135
- PMCID: PMC6505066
- DOI: 10.1186/s12874-019-0740-x
Veterans Affairs patient database (VAPD 2014-2017): building nationwide granular data for clinical discovery
Abstract
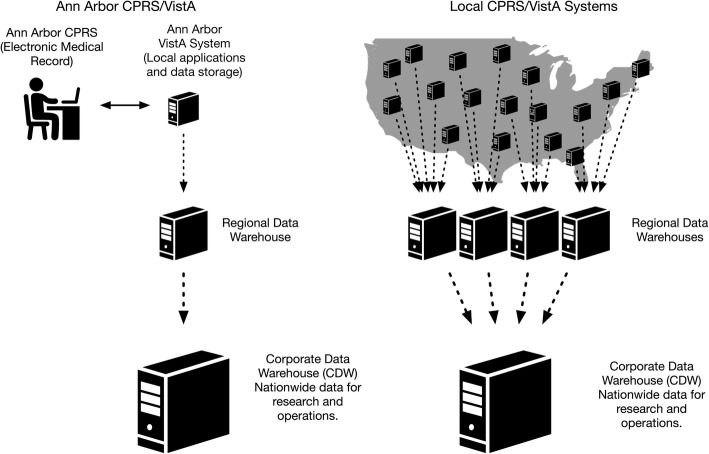
Background: To study patient physiology throughout a period of acute hospitalization, we sought to create accessible, standardized nationwide data at the level of the individual patient-facility-day. This methodology paper summarizes the development, organization, and characteristics of the Veterans Affairs Patient Database 2014-2017 (VAPD 2014-2017). The VAPD 2014-2017 contains acute hospitalizations from all parts of the nationwide VA healthcare system with daily physiology including clinical data (labs, vitals, medications, risk scores, etc.), intensive care unit (ICU) indicators, facility, patient, and hospitalization characteristics.
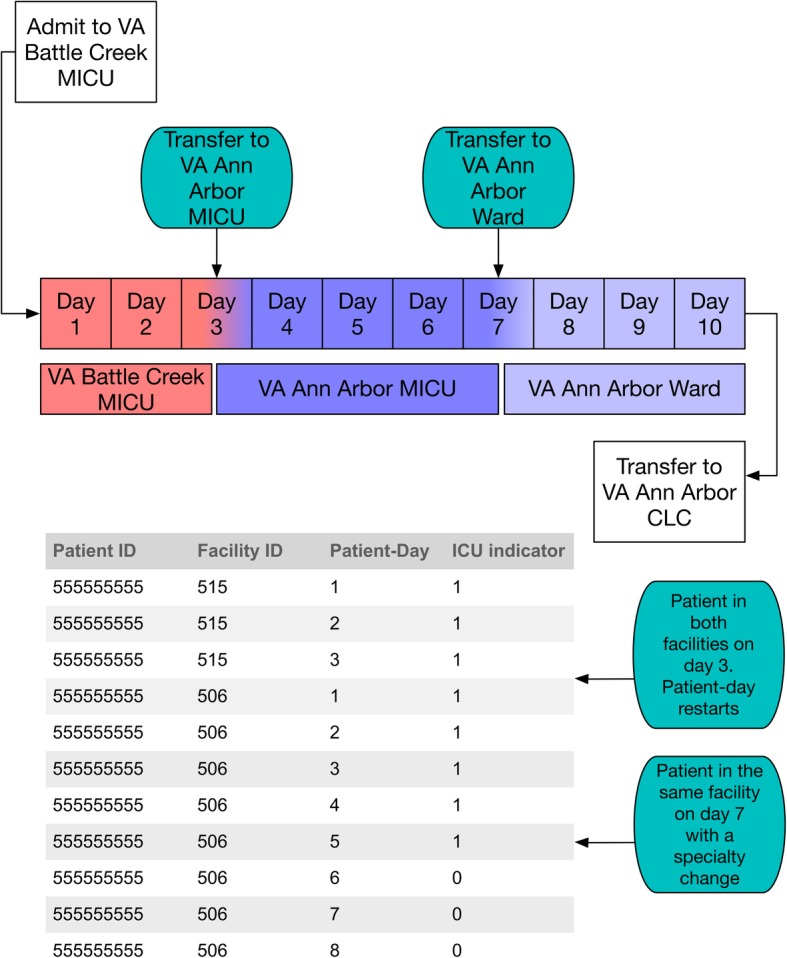
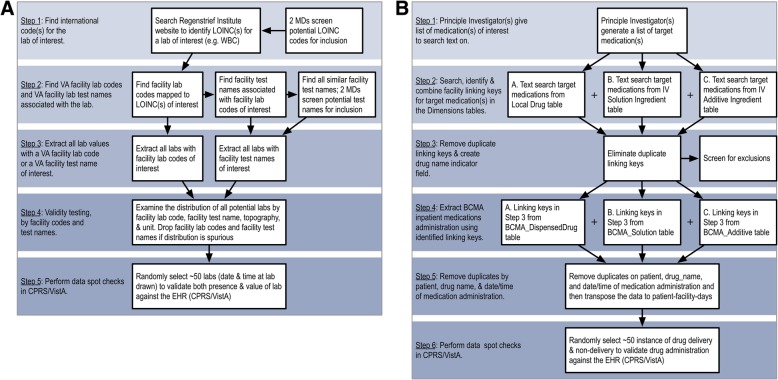
Methods: The VA data structure and database organization represents a complex multi-hospital system. We define a single-site hospitalization as one or more consecutive stays with an acute treating specialty at a single facility. The VAPD 2014-2017 is structured at the patient-facility-day level, where every patient-day in a hospital is a row with separate identification variables for facility, patient, and hospitalization. The VAPD 2014-2017 includes daily laboratory, vital signs, and inpatient medication. Such data were validated and verified through lab value range and comparison with patient charts. Sepsis, risk scores, and organ dysfunction definitions were standardized and calculated.
Results: We identified 565,242 single-site hospitalizations (SSHs) in 2014; 558,060 SSHs in 2015; 553,961 SSHs in 2016; and 550,236 SSHs in 2017 at 141 VA hospitals. The average length of stay was four days for all study years. In-hospital mortality decreased from 2014 to 2017 (1.7 to 1.4%), 30-day readmission rates increased from 15.3% in 2014 to 15.6% in 2017; 30-day mortality also decreased from 4.4% in 2014 to 4.1% in 2017. From 2014 to 2017, there were 107,512 (4.8%) of SSHs that met the Center for Disease Control and Prevention's Electronic Health Record-based retrospective definition of sepsis.
Conclusion: The VAPD 2014-2017 represents a large, standardized collection of granular data from a heterogeneous nationwide healthcare system. It is also a direct resource for studying the evolution of inpatient physiology during both acute and critical illness.
Keywords: Electronic health records; Healthcare database; Hospitalization, sepsis; Laboratory values; Patient physiology.
Conflict of interest statement
Ethics approval and consent to participate
VA Ann Arbor Healthcare System Institutional Review Board and the IRB approval number for the project: IRB-2016-326.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- CCMRcodes/VAPD [https://github.com/CCMRcodes/VAPD ]. Accessed 6 Mar 2018
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
