

Peritoneal Dialysis-Associated Peritonitis
- PMID: 31068338
- PMCID: PMC6625612
- DOI: 10.2215/CJN.14631218
Peritoneal Dialysis-Associated Peritonitis
Abstract
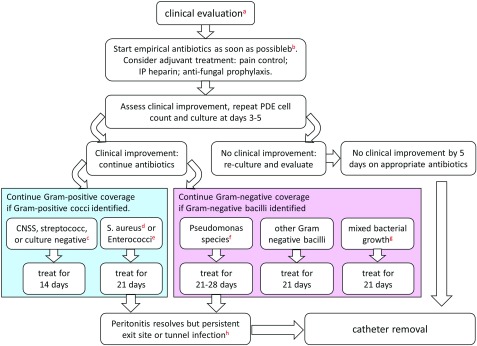
Peritonitis is a common and severe complication in peritoneal dialysis (PD). Detailed recommendations on the prevention and treatment of PD-associated peritonitis have been published by the International Society for Peritoneal Dialysis (ISPD), but there is a substantial variation in clinical practice among dialysis units. Prophylactic antibiotics administered before PD catheter insertion, colonoscopy, or invasive gynecologic procedures, daily topical application of antibiotic cream or ointment to the catheter exit site, and prompt treatment of exit site or catheter infection are key measures to prevent PD-associated peritonitis. When a patient on PD presents with clinical features compatible with PD-associated peritonitis, empirical antibiotic therapy, with coverage of both Gram-positive and Gram-negative organisms (including Pseudomonas species), should be started once the appropriate microbiologic specimens have been obtained. Intraperitoneal is the preferred route of administration. Antifungal prophylaxis, preferably oral nystatin, should be added to prevent secondary fungal peritonitis. Once the PD effluent Gram stain or culture and sensitivity results are available, antibiotic therapy can be adjusted accordingly. A detailed description on the dosage of individual antibiotic can be found in the latest recommendations by the ISPD. The duration of antibiotics is usually 2-3 weeks, depending on the specific organisms identified. Catheter removal and temporary hemodialysis support is recommended for refractory, relapsing, or fungal peritonitis. In some patients, a new PD catheter could be inserted after complete resolution of the peritonitis. PD catheter removal should also be considered for refractory exit site or tunnel infections. After the improvement in clinical practice, there is a worldwide trend of reduction in PD-associated peritonitis rate, supporting the use of PD as a first-line dialysis modality.
Keywords: Antibiotic; Infection; Peritonitis; dialysis; end-stage renal disease; microbiology; peritoneal dialysis.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Szeto CC, Wong TY, Chow KM, Leung CB, Li PK: Are peritoneal dialysis patients with and without residual renal function equivalent for survival study? Insight from a retrospective review of the cause of death. Nephrol Dial Transplant 18: 977–982, 2003 - PubMed
-
- Htay H, Cho Y, Pascoe EM, Darssan D, Nadeau-Fredette AC, Hawley C, Clayton PA, Borlace M, Badve SV, Sud K, Boudville N, McDonald SP, Johnson DW: Multicenter registry analysis of center characteristics associated with technique failure in patients on incident peritoneal dialysis. Clin J Am Soc Nephrol 12: 1090–1099, 2017 - PMC - PubMed
-
- Li PK, Szeto CC, Piraino B, Bernardini J, Figueiredo AE, Gupta A, Johnson DW, Kuijper EJ, Lye WC, Salzer W, Schaefer F, Struijk DG; International Society for Peritoneal Dialysis: Peritoneal dialysis-related infections recommendations: 2010 update. Perit Dial Int 30: 393–423, 2010 - PubMed
-
- Piraino B, Bernardini J, Brown E, Figueiredo A, Johnson DW, Lye WC, Price V, Ramalakshmi S, Szeto CC: ISPD position statement on reducing the risks of peritoneal dialysis-related infections. Perit Dial Int 31: 614–630, 2011 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
