

Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia
- PMID: 31068690
- PMCID: PMC7136170
- DOI: 10.1038/s41581-019-0152-5
Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia
Abstract
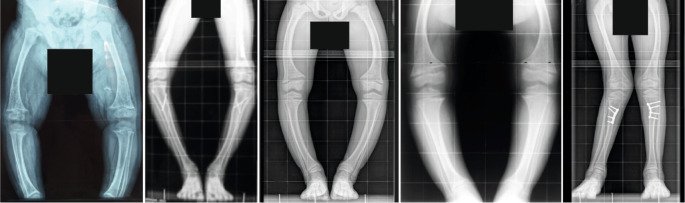
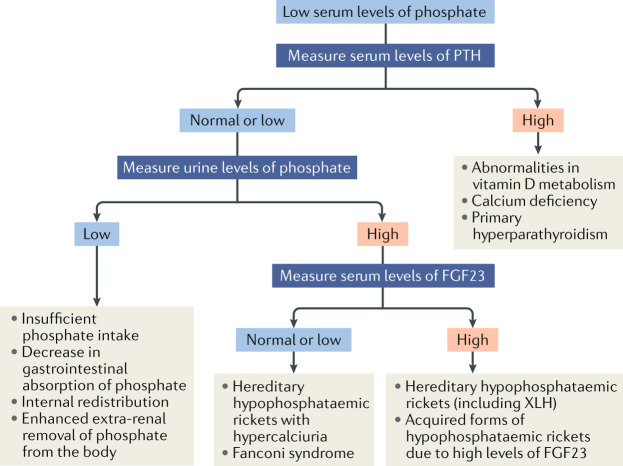
X-linked hypophosphataemia (XLH) is the most common cause of inherited phosphate wasting and is associated with severe complications such as rickets, lower limb deformities, pain, poor mineralization of the teeth and disproportionate short stature in children as well as hyperparathyroidism, osteomalacia, enthesopathies, osteoarthritis and pseudofractures in adults. The characteristics and severity of XLH vary between patients. Because of its rarity, the diagnosis and specific treatment of XLH are frequently delayed, which has a detrimental effect on patient outcomes. In this Evidence-Based Guideline, we recommend that the diagnosis of XLH is based on signs of rickets and/or osteomalacia in association with hypophosphataemia and renal phosphate wasting in the absence of vitamin D or calcium deficiency. Whenever possible, the diagnosis should be confirmed by molecular genetic analysis or measurement of levels of fibroblast growth factor 23 (FGF23) before treatment. Owing to the multisystemic nature of the disease, patients should be seen regularly by multidisciplinary teams organized by a metabolic bone disease expert. In this article, we summarize the current evidence and provide recommendations on features of the disease, including new treatment modalities, to improve knowledge and provide guidance for diagnosis and multidisciplinary care.
Conflict of interest statement
J.B. receives support for research and consultancy from Kyowa Kirin. A.L. receives research support from Kyowa Kirin. D.H. receives a research grant and speaker and consultant fees from Kyowa Kirin. F.E., E.L., P.K., K.B., D.S. and K.B. receive consultation fees from Kyowa Kirin. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
