

Case Reports
doi: 10.1038/s41591-019-0437-z.
Epub 2019 May 8.
Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus
Affiliations
- PMID: 31068712
- PMCID: PMC6557439
- DOI: 10.1038/s41591-019-0437-z
Item in Clipboard
Case Reports
Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus
Nat Med.
2019 May.
Abstract
A 15-year-old patient with cystic fibrosis with a disseminated Mycobacterium abscessus infection was treated with a three-phage cocktail following bilateral lung transplantation. Effective lytic phage derivatives that efficiently kill the infectious M. abscessus strain were developed by genome engineering and forward genetics. Intravenous phage treatment was well tolerated and associated with objective clinical improvement, including sternal wound closure, improved liver function, and substantial resolution of infected skin nodules.
Conflict of interest statement
Competing Interests
Dr. Schooley serves as an uncompensated member of the AmpliPhi Scientific Advisory Board. Other authors declare no competing interests.
Figures
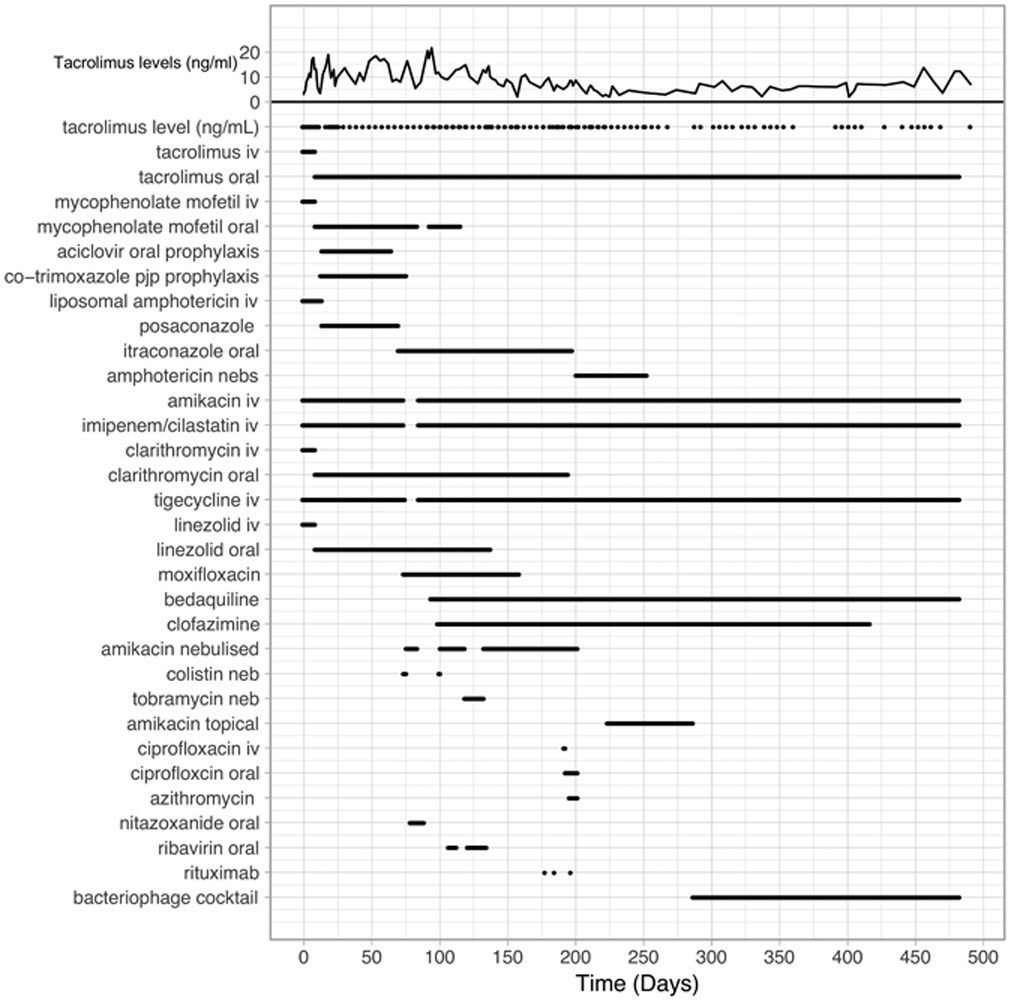
Timeline showing administration of antibiotics, immunosuppressive drugs, and the phage cocktail. Levels of the immunosuppressive drug Tacrolimus are shown at the top, and the administration of drugs is as indicated.

Genes are shown as colored boxes above or below a genome track, reflecting rightwards and leftwards transcription, respectively. Pairwise nucleotide sequence similarity is indicated by spectrum-colored shading between genomes, with violet representing closest similarity.
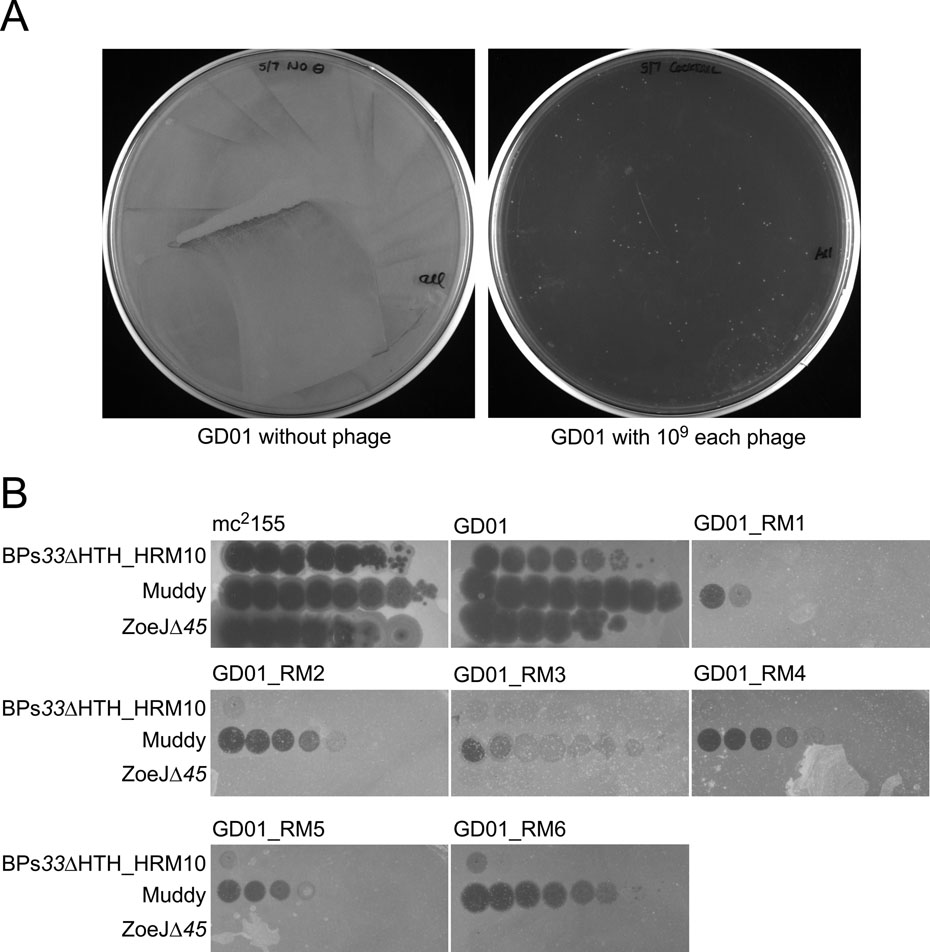
A. Approximately 5 × 108 cells of M. abscessus GD01 in one ml were incubated with a cocktail of 109 pfu each of three phages for one week in liquid culture. Aliquots (100 μl) were plated onto solid media and incubated at 37° C. In the absence of phage, a confluent lawn grew (left), and in the presence of phage (right), approximately 150 small colonies were observed. B. Six individual colonies were picked, grown and retested for phage susceptibilities. Top agar overlays with each strain were plated on solid media and 10-fold serial dilutions of phages (as indicated) were spotted onto each plate.
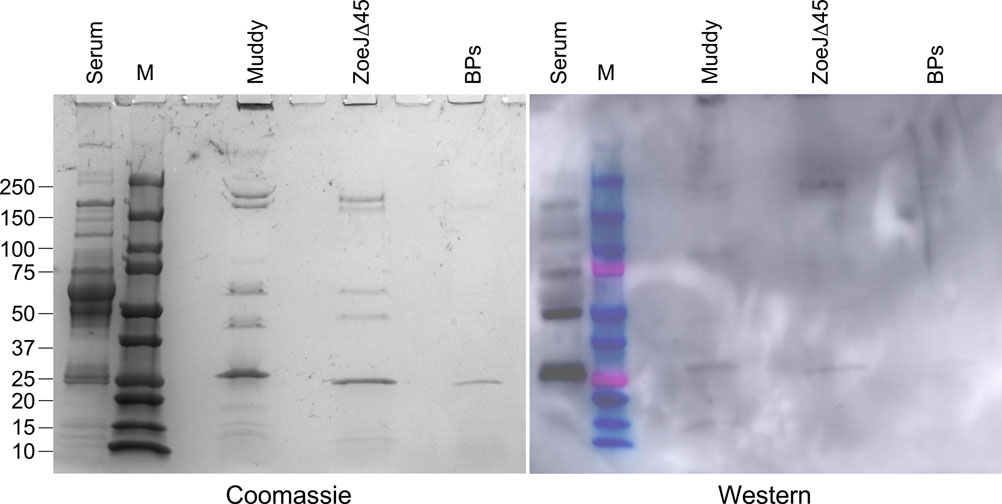
Phage preparations of Muddy, ZoeJD45, and BPs33DHTH-HRM10 (as shown) each containing approximately 2 × 1010 phage particles were separated by SDS-PAGE, together with protein markers (M) and a control sample of 10 μl of a 1:100 dilution of patient serum (serum) collected 72 days after initiation of phage treatment. The gel was stained with Coomassie Blue (left), transferred to a membrane for a Western blot which was probed with the same patient serum and an anti-human Horse Radish Peroxidase conjugated secondary antibody. These assays were repeated three times with similar results; a representative experiment is shown.
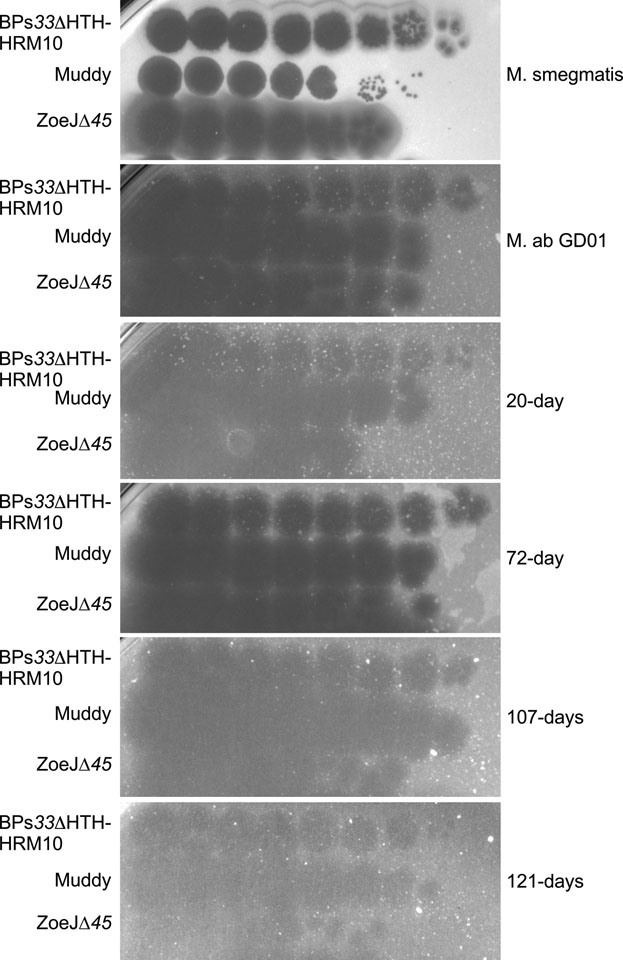
M. abscessus were recovered at 20-, 72-, 107, and 121-days after initiation of phage treatment, propagated, and tested for susceptibilities to each of the phages in the cocktail. Each phage was diluted serially 10-fold and spotted onto bacterial lawns. These assays were repeat at least twice with similar results; a representative experiment is shown.
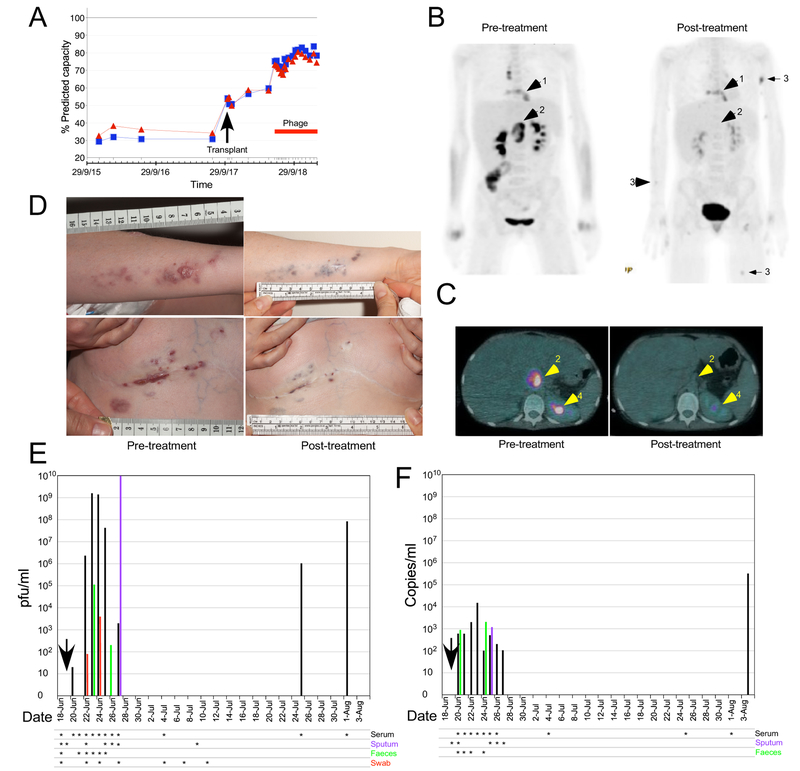
A. Lung function as percent Predicted Forced Expiratory Volume in One Second (FEV1; blue) and Forced Vital Capacity (FVC; red). Whole body (B) and cross-section (C) PET-CT scans twelve weeks before and six weeks post-phage treatment. Arrows show (1) the sternal area and surrounding soft tissue, (2) abdominal lymph nodes at the porta-hepatis, and (3) skin nodules, respectively. Arrow 4 indicates normal kidney excretion. D. Upper and lower panels show the patient’s left arm and sternal wound, respectively, immediately prior to and six months after phage treatment. E and F. Phage titers by plaque assay (E) or dPCR (F) following phage administration (vertical arrow). Serum (black bars), sputum (purple bars), feces (green bars), and wound swab (red bars) were tested on the dates indicated (asterisks).
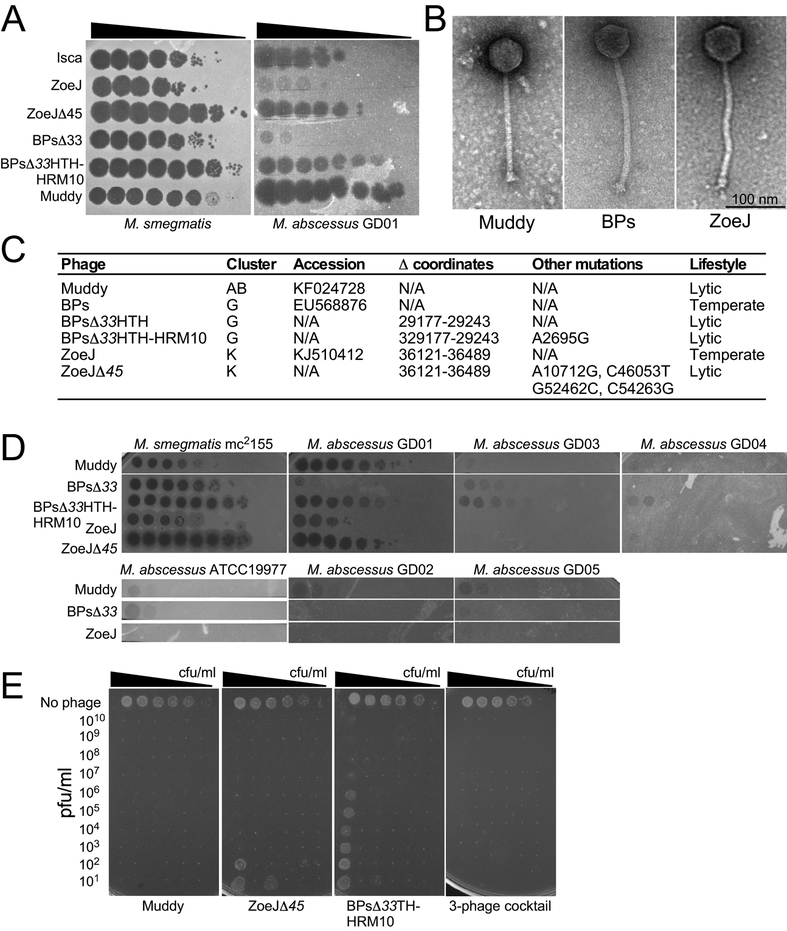
A. Phage lysates were serially diluted 10-fold and spotted onto M. smegmatis mc2155 and M. abscessus GD01 lawns. These assays were repeated at least ten times with similar results and a representative experiment is shown. B. Electron micrographs of phages Muddy, BPs, and ZoeJ. Representative images are shown. C. Key characteristics of phages. D. Phages were serially diluted 10-fold and spotted onto mycobacteria as indicated. These assays were repeated at least twice with similar results and representative experiments are shown. E.
M. abscessus GD01 (~108 cfu/ml) was serially diluted 10-fold in 11 replicates, and either no phage or phage added at indicated concentrations. Cultures were incubated at 37°C for 24 hrs and 3 μl aliquots plated onto solid media and incubated for 7 days. These assays were repeated at least three times with similar results and a representative experiment is shown.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
