

Assessment of the Rate of Skip Metastasis to Neck Level IV in Patients With Clinically Node-Negative Neck Oral Cavity Squamous Cell Carcinoma: A Systematic Review and Meta-analysis
- PMID: 31070693
- PMCID: PMC6512277
- DOI: 10.1001/jamaoto.2019.0784
Assessment of the Rate of Skip Metastasis to Neck Level IV in Patients With Clinically Node-Negative Neck Oral Cavity Squamous Cell Carcinoma: A Systematic Review and Meta-analysis
Abstract
Importance: The rate of skip metastasis to neck level IV in patients with clinically node-negative neck (cN0) oral cavity squamous cell carcinoma (OCSCC) remains controversial.
Objective: To provide a high level of evidence using a meta-analysis on the rate of skip metastasis to level IV in this subset of patients.
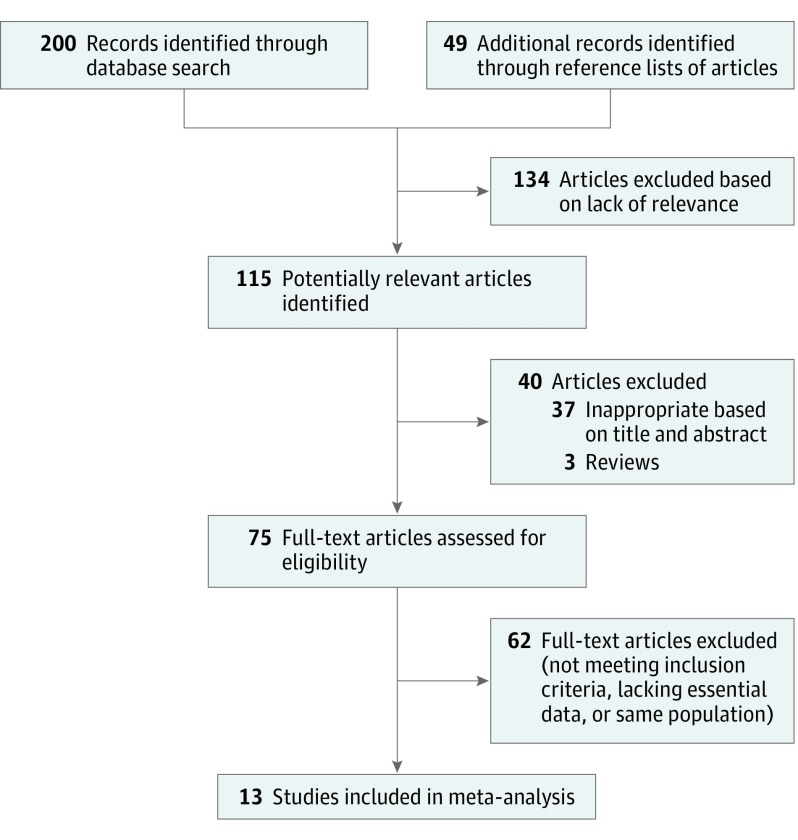
Data sources: The Embase, PubMed, and Google Scholar databases were searched for articles published during the period of January 1, 1970, through December 31, 2017, using the following key terms: neck dissection, N0 neck, squamous cell carcinoma, skip metastasis, radical neck dissection, lymph node management, neck metastasis, oral cavity cancer, and tongue cancer. Some terms were also used in combination, and the reference section of each article was searched for additional potentially relevant publications. Data were analyzed from January 8 through 11, 2018.
Study selection: Inclusion criteria were all cohorts, including from any randomized clinical trial, case-control study, case study, and case report; studies of patients with the histopathologic diagnosis of OCSCC; and studies that differentiated data between skip metastasis and sequential metastasis to neck level IV. Of the 115 articles retrieved from the literature, 11 retrospective studies and 2 prospective randomized clinical trials (n = 1359 patients) were included.
Data extraction and synthesis: Meta-analysis of Observational Studies in Epidemiology guidelines were followed. Fixed-effects model and 95% CIs were estimated, and data of included studies were pooled using a fixed-effects model.
Main outcomes and measures: Overall proportion of neck involvement and the rate of level IV skip metastasis. Subgroup analysis for primary site and tumor staging.
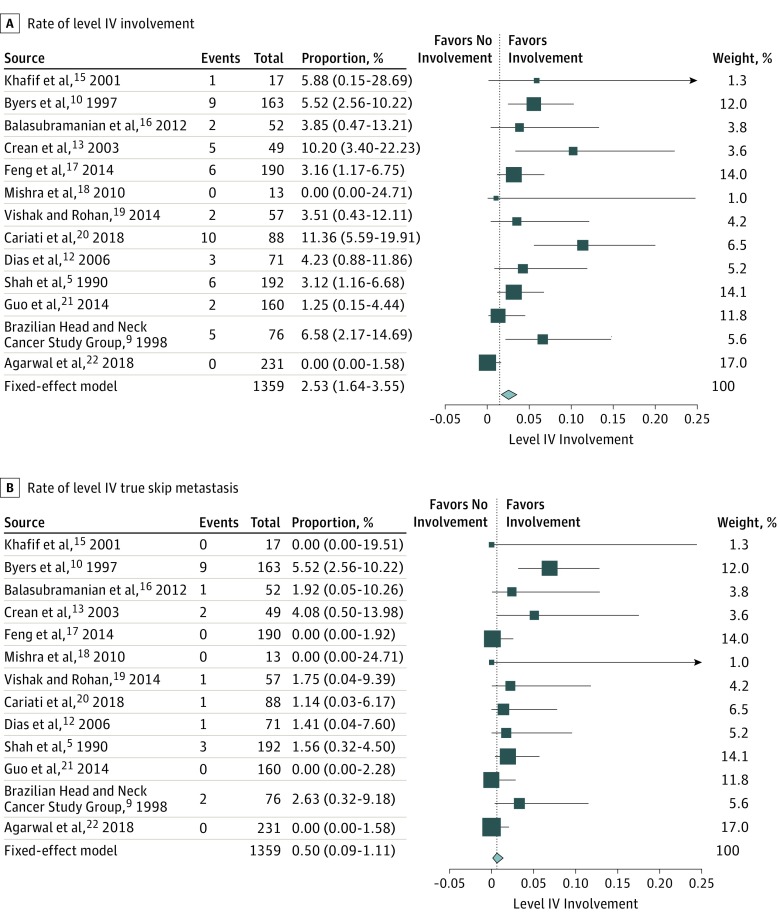
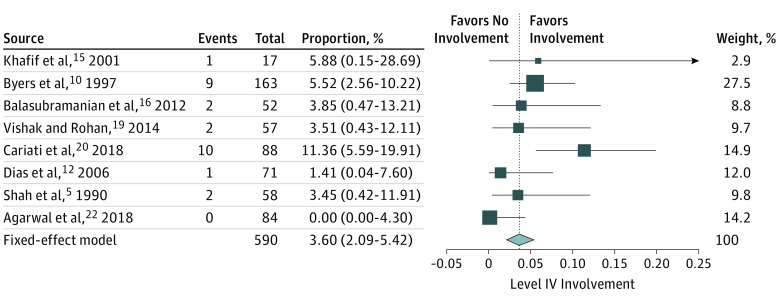
Results: The rate of level IV involvement in patients with cN0 ranged between 0% and 11.40% with a fixed-effects model of 2.53% (95% CI, 1.64%-3.55%). The rate of skip metastasis ranged from 0% to 5.50% with a fixed-effects model of 0.50% (95% CI, 0.09%-1.11%). The rate of level IV skip metastasis did not increase significantly in cases that involved neck levels I through III. Tumor staging and primary site tumor did not significantly affect the rate of skip metastasis.
Conclusions and relevance: This meta-analysis showed very low rates of skip metastasis to neck level IV in patients diagnosed with cN0 OCSCC. Encountering an allegedly positive lymph node during neck dissection does not portend high rates of level IV involvement. Supraomohyoid neck dissection is therefore adequate for this subset of patients.
Conflict of interest statement
Figures
Comment in
-
Inclusion of Neck Level IV in Treatment of Patients With Clinically Node-Negative Oral Cavity Cancer.JAMA Otolaryngol Head Neck Surg. 2019 Jun 1;145(6):548-549. doi: 10.1001/jamaoto.2019.0785. JAMA Otolaryngol Head Neck Surg. 2019. PMID: 31070695 No abstract available.
-
Supraomohyoid Neck Dissection for the Clinically Node-Negative Neck in Oral Cavity Squamous Cell Carcinoma: Time to Change Practices?JAMA Otolaryngol Head Neck Surg. 2020 Jan 1;146(1):85. doi: 10.1001/jamaoto.2019.3404. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 31697346 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
