

Associations Among End-of-Life Discussions, Health-Care Utilization, and Costs in Persons With Advanced Cancer: A Systematic Review
- PMID: 31072109
- PMCID: PMC6711813
- DOI: 10.1177/1049909119848148
Associations Among End-of-Life Discussions, Health-Care Utilization, and Costs in Persons With Advanced Cancer: A Systematic Review
Abstract
Background: Aggressive end-of-life (EOL) care is associated with lower quality of life and greater regret about treatment decisions. Higher EOL costs are also associated with lower quality EOL care. Advance care planning and goals-of-care conversations ("EOL discussions") may influence EOL health-care utilization and costs among persons with cancer.
Objective: To describe associations among EOL discussions, health-care utilization and place of death, and costs in persons with advanced cancer and explore variation in study measures.
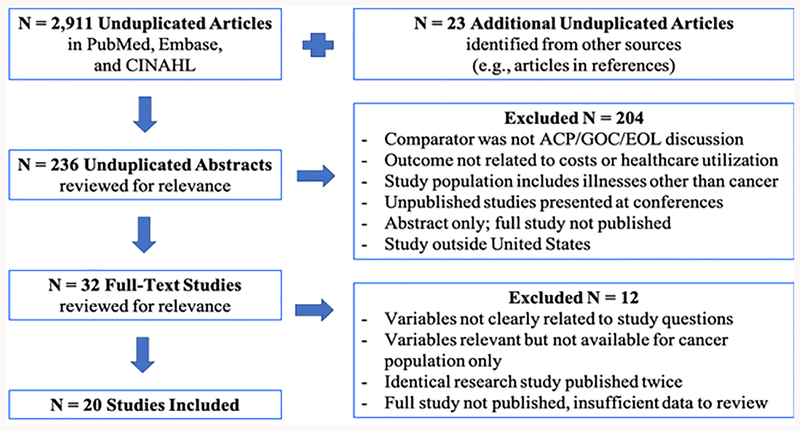
Methods: A systematic review was conducted using PubMed, Embase, and CINAHL. Twenty quantitative studies published between January 2012 and January 2019 were included.
Results: End-of-life discussions are associated with lower health-care costs in the last 30 days of life (median US$1048 vs US$23482; P < .001); lower likelihood of acute care at EOL (odds ratio [(OR] ranging 0.43-0.69); lower likelihood of intensive care at EOL (ORs ranging 0.26-0.68); lower odds of chemotherapy near death (ORs 0.41, 0.57); lower odds of emergency department use and shorter length of hospital stay; greater use of hospice (ORs ranging 1.79 to 6.88); and greater likelihood of death outside the hospital. Earlier EOL discussions (30+ days before death) are more strongly associated with less aggressive care outcomes than conversations occurring near death.
Conclusions: End-of-life discussions are associated with less aggressive, less costly EOL care. Clinicians should initiate these discussions with patients having cancer earlier to better align care with preferences.
Keywords: advance care planning; cancer; communication; costs; decision-making; end of life; goals of care; health-care utilization; systematic review.
Figures
References
-
- Lopez-Acevedo M, Havrilesky LJ, Broadwater G, et al. Timing of end-of-life care discussion with performance on end-of-life quality indicators in ovarian cancer. Gynecol Oncol. 2013;130(1):156–161. - PubMed
-
- Gieniusz M, Nunes R, Saha V, Renson A, Schubert F, Carey J. Earlier Goals of Care Discussions in Hospitalized Terminally Ill Patients and the Quality of End-of-Life Care: A Retrospective Study. Am J Hosp Palliat Care. 2018;35(1):21–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
