

Robotic assisted-bronchoscopy: technical tips and lessons learned from the initial experience with sampling peripheral lung lesions
- PMID: 31072355
- PMCID: PMC6506952
- DOI: 10.1186/s12890-019-0857-z
Robotic assisted-bronchoscopy: technical tips and lessons learned from the initial experience with sampling peripheral lung lesions
Abstract
Background: Peripheral pulmonary nodules are increasingly detected in patients screened for lung cancer or during disease progression of thoracic or extrathoracic malignancies. Sampling these lesions requires surgery, computed tomography (CT)-guided biopsy or bronchoscopic interventions. Bronchoscopic interventions are preferable because they have lower complications and often patients may not be ideal candidates for surgical or CT-guided biopsy. In addition, guidelines recommend diagnosis and staging in one single procedure. The diagnostic yield of existing advanced bronchoscopic techniques including electromagnetic navigation, radial probe ultrasonography, ultrathin bronchoscopy or virtual bronchoscopy remains suboptimal. The purpose of this paper is to codify the technique whereby a diagnostic bronchoscopy is performed using the new robotic platform.
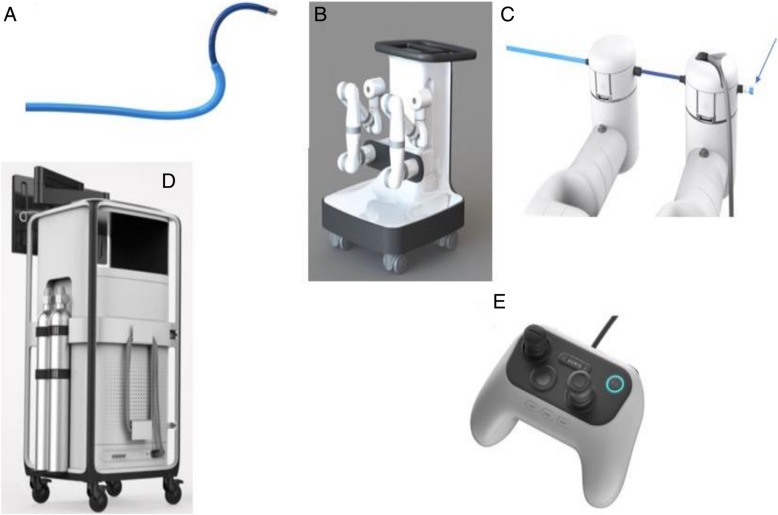
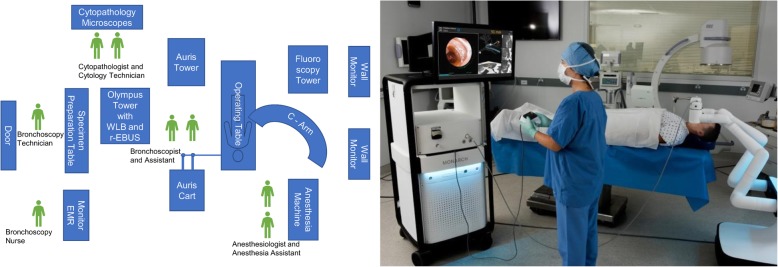
Methods: In the present report, I describe the technique for performing robotic-assisted bronchoscopy (RAB) using the Monarch™ platform (Auris Health, Inc., Redwood City, CA).
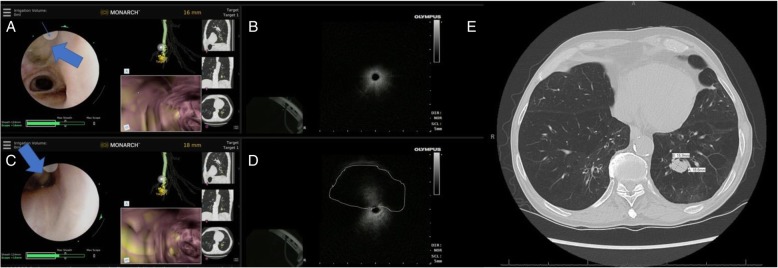
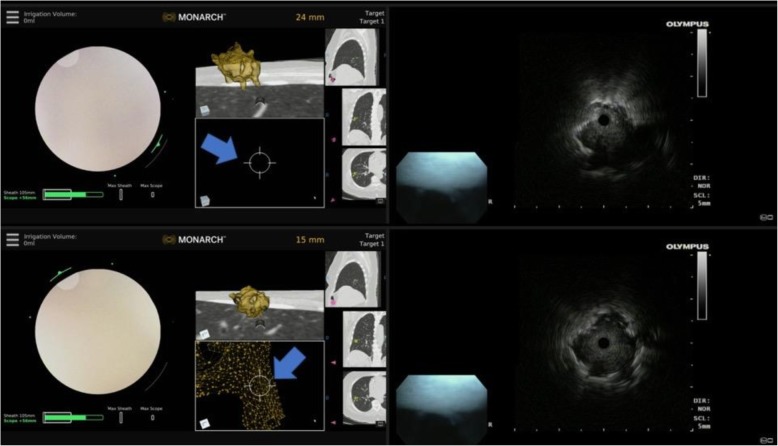
Results: Appropriate team training, patient selection, anesthesia settings, optimal tissue acquisition and processing, and prevention of complications are described and illustrated.
Conclusions: RAB may be beneficial for patients with peripheral lung lesions that require biopsy prior to surgical resection, stereotactic radiation, targeted or immunotherapy.
Keywords: Guided bronchoscopy; Lung cancer; Navigation bronchoscopy; Peripheral lung lesion; Peripheral lung nodule; Radial probe ultrasound; Robotic bronchoscopy; Screening.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable- no personal information is provided in your manuscript.
Competing interests
The author declares that he has no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Gould MK, Donington J, Lynch WR, Mazzone PJ, Midthun DE, Naidich DP, et al. Evaluation of individuals with pulmonary nodules: when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e93S–e120S. doi: 10.1378/chest.12-2351. - DOI - PMC - PubMed
-
- Silvestri GA, Gonzalez AV, Jantz MA, Margolis ML, Gould MK, Tanoue LT, et al. Methods for staging non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e211S–e250S. doi: 10.1378/chest.12-2355. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
