

Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review
- PMID: 31072578
- PMCID: PMC6538508
- DOI: 10.1016/j.jacc.2019.02.045
Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review
Abstract
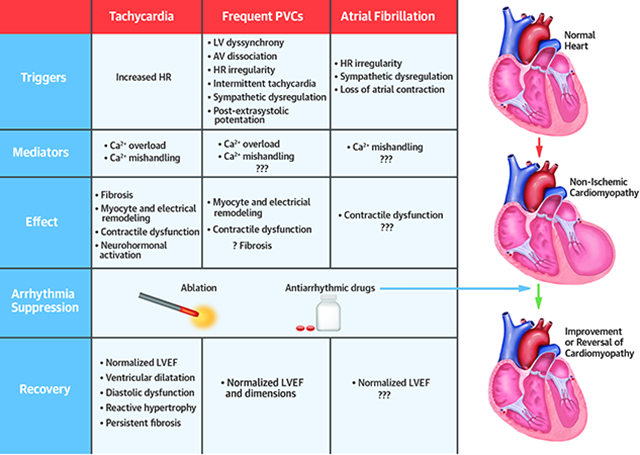
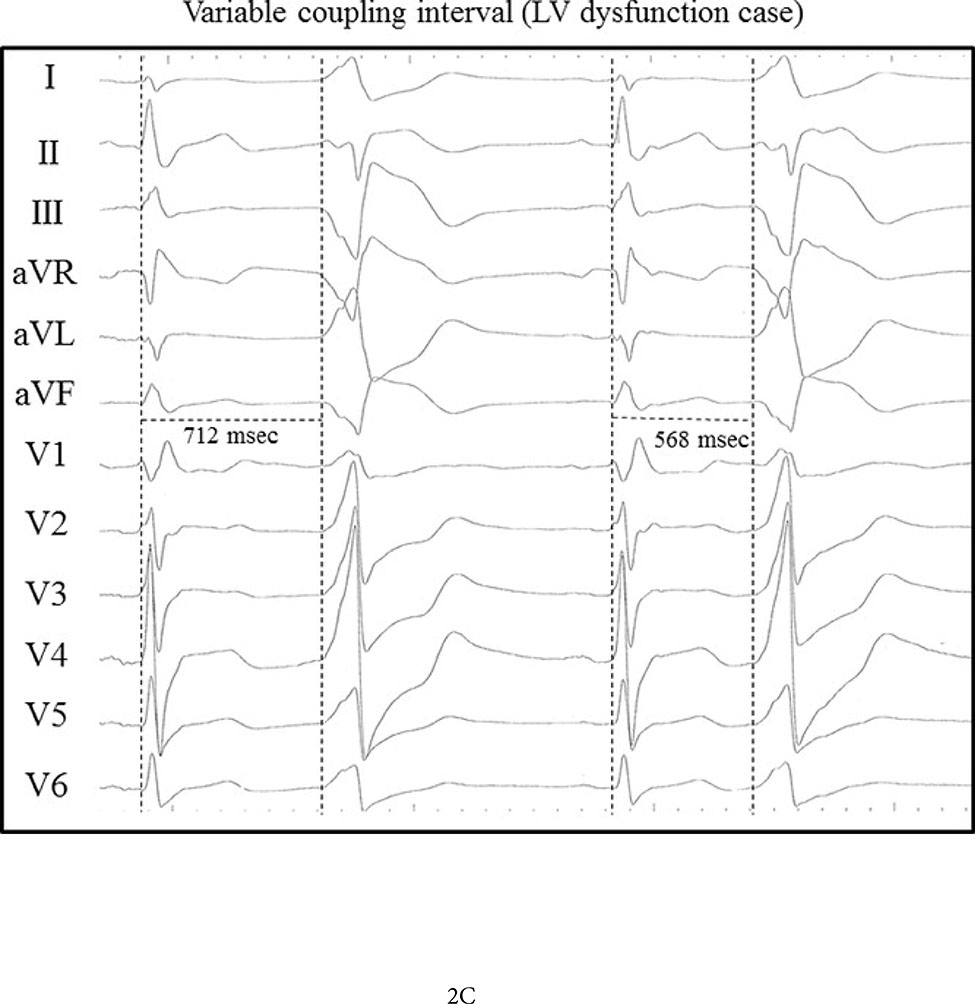
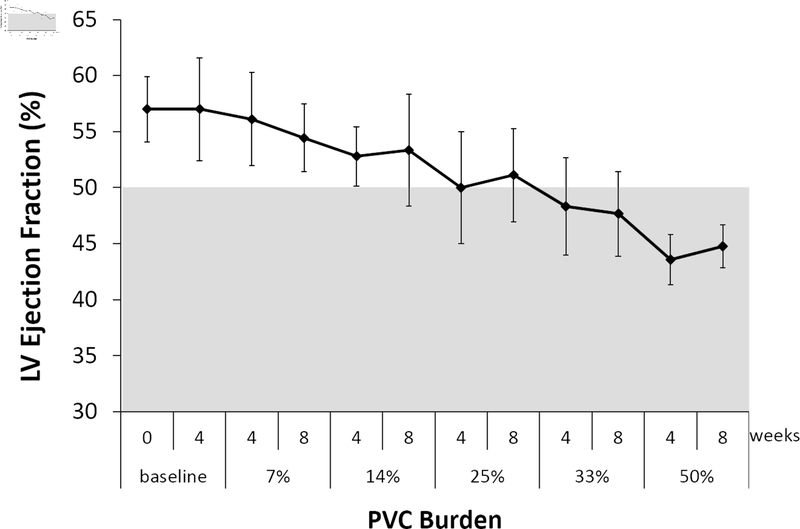
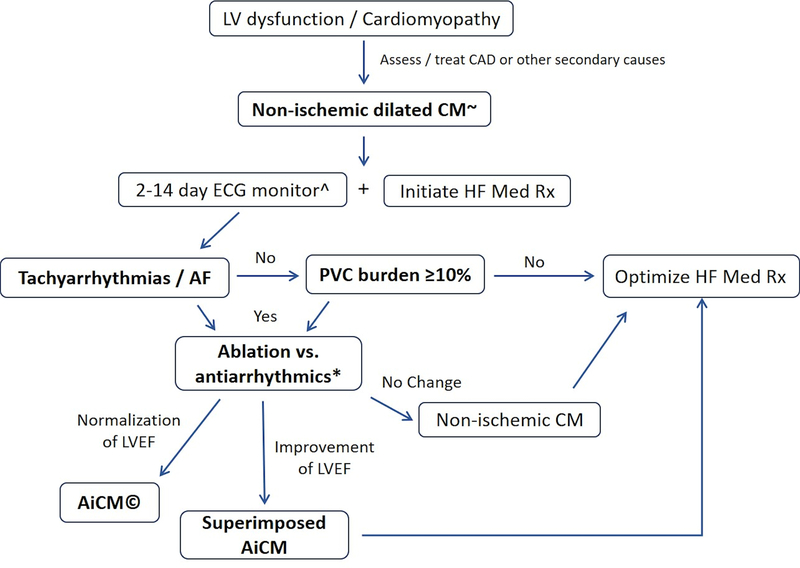
Arrhythmias coexist in patients with heart failure (HF) and left ventricular (LV) dysfunction. Tachycardias, atrial fibrillation, and premature ventricular contractions are known to trigger a reversible dilated cardiomyopathy referred as arrhythmia-induced cardiomyopathy (AiCM). It remains unclear why some patients are more prone to develop AiCM despite similar arrhythmia burdens. The challenge is to determine whether arrhythmias are fully, partially, or at all responsible for an observed LV dysfunction. AiCM should be suspected in patients with mean heart rate >100 beats/min, atrial fibrillation, and/or premature ventricular contractions burden ≥10%. Reversal of cardiomyopathy by elimination of the arrhythmia confirms AiCM. Therapeutic choice depends on the culprit arrhythmia, patient comorbidities, and preferences. Following recovery of LV function, patients require continued follow-up if an abnormal myocardial substrate is present. Appropriate diagnosis and treatment of AiCM is likely to improve quality of life and clinical outcomes and to reduce hospital admission and health care spending.
Keywords: arrhythmia; cardiomyopathy; heart failure; left ventricular dysfunction; premature ventricular contractions; supraventricular tachycardia.
Published by Elsevier Inc.
Figures
References
-
- Bozkurt B, Colvin M, Cook J et al. Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement From the American Heart Association. Circulation 2016;134:e579–e646. - PubMed
-
- Trulock KM, Narayan SM, Piccini JP. Rhythm control in heart failure patients with atrial fibrillation: contemporary challenges including the role of ablation. J Am Coll Cardiol 2014;64:710–21. - PubMed
-
- Marrouche NF, Brachmann J, Andresen D et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N Engl J Med 2018;378:417–427. - PubMed
-
- Fazio G, Mongiovi M, Sutera L, Novo G, Novo S, Pipitone S. Segmental dyskinesia in Wolff-Parkinson-White syndrome: a possible cause of dilatative cardiomyopathy. Int J Cardiol 2008;123:e31–4. - PubMed
-
- Gossage AMBHJ. On auricular fibrillation. Quarterly Journal of Medicine 1913;6:435–440.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
