

Estimates of the 2016 global burden of kidney disease attributable to ambient fine particulate matter air pollution
- PMID: 31072847
- PMCID: PMC6528010
- DOI: 10.1136/bmjopen-2018-022450
Estimates of the 2016 global burden of kidney disease attributable to ambient fine particulate matter air pollution
Abstract
Objective: To quantitate the 2016 global and national burden of chronic kidney disease (CKD) attributable to ambient fine particulate matter air pollution ≤ 2.5 μm in aerodynamic diameter (PM2.5).
Design: We used the Global Burden of Disease (GBD) study data and methodologies to estimate the 2016 burden of CKD attributable to PM2.5 in 194 countries and territories. Population-weighted PM2.5 levels and incident rates of CKD for each country were curated from the GBD study publicly available data sources.
Setting: GBD global and national data on PM2.5 and CKD.
Participants: 194 countries and territories.
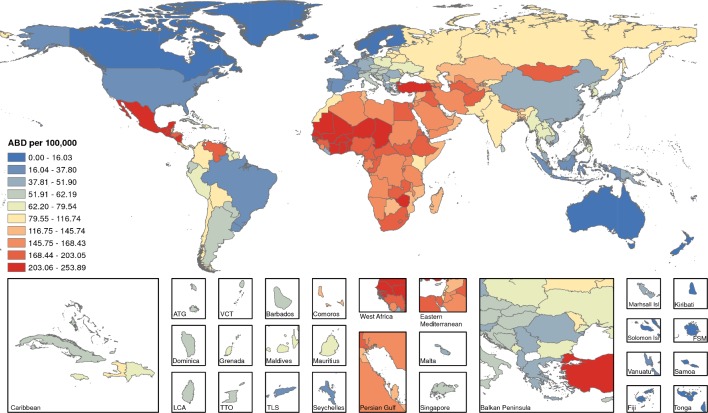
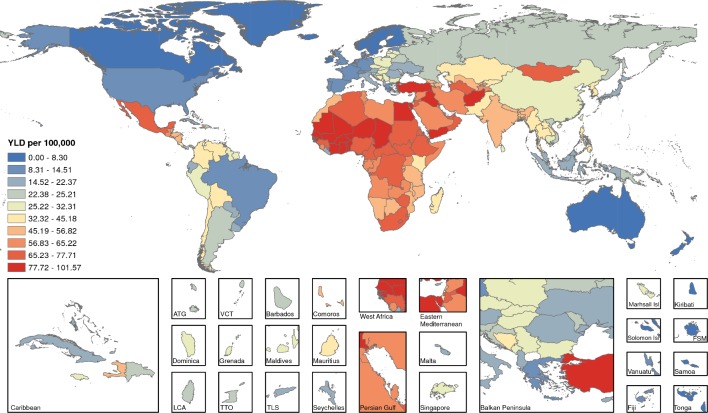
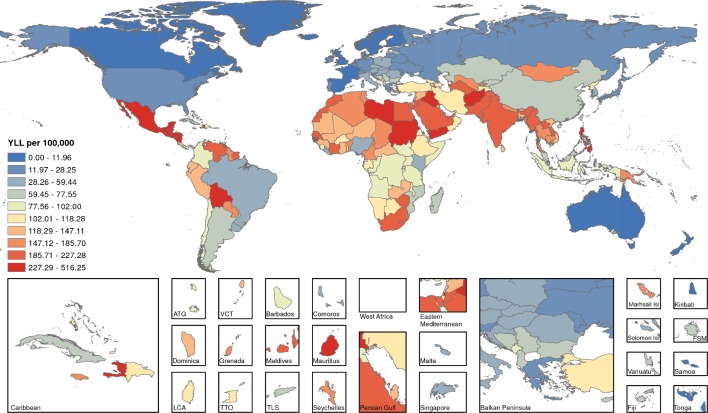
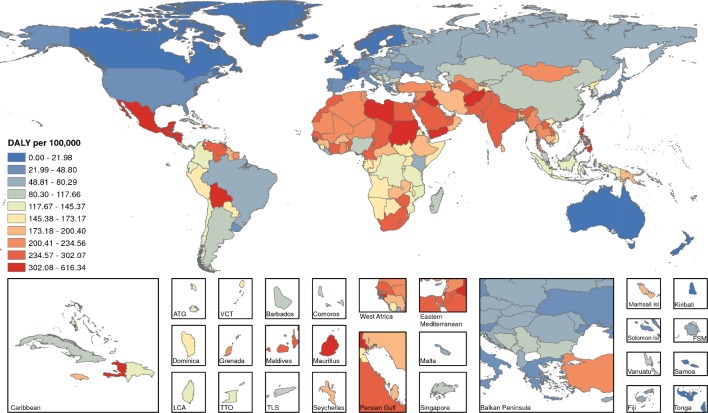
Main outcome measures: We estimated the attributable burden of disease (ABD), years living with disability (YLD), years of life lost (YLL) and disability-adjusted life-years (DALYs).
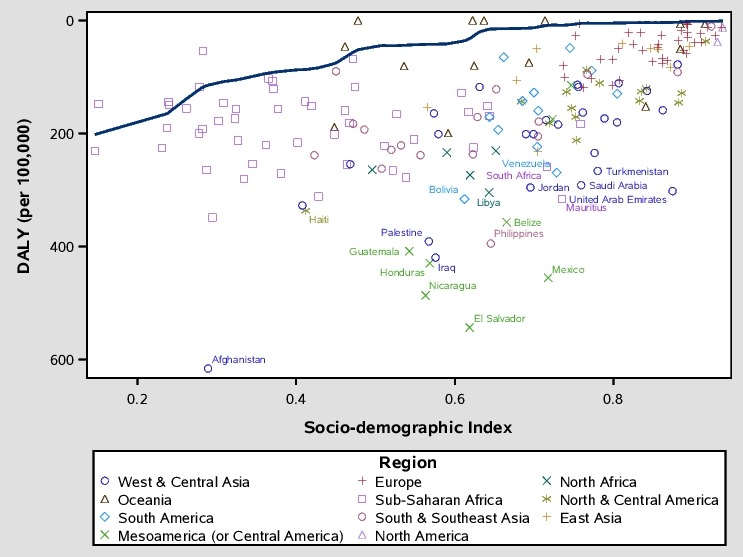
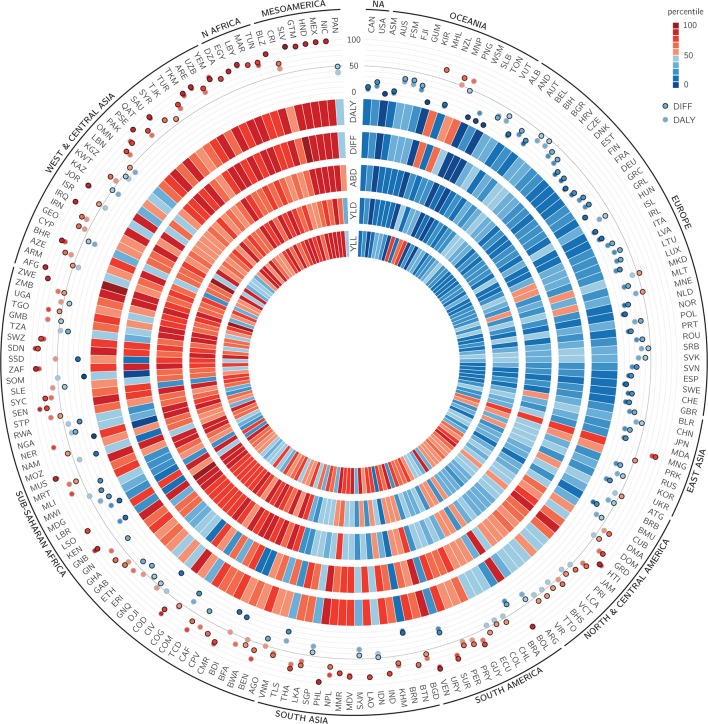
Results: The 2016 global burden of incident CKD attributable to PM2.5 was 6 950 514 (95% uncertainty interval: 5 061 533-8 914 745). Global YLD, YLL and DALYs of CKD attributable to PM2.5 were 2 849 311 (1 875 219-3 983 941), 8 587 735 (6 355 784-10 772 239) and 11 445 397 (8 380 246-14 554 091), respectively. Age-standardised ABD, YLL, YLD and DALY rates varied substantially among geographies. Populations in Mesoamerica, Northern Africa, several countries in the Eastern Mediterranean region, Afghanistan, Pakistan, India and several countries in Southeast Asia were among those with highest age-standardised DALY rates. For example, age-standardised DALYs per 100 000 were 543.35 (391.16-707.96) in El Salvador, 455.29 (332.51-577.97) in Mexico, 408.41 (283.82-551.84) in Guatemala, 238.25 (173.90-303.98) in India and 178.26 (125.31-238.47) in Sri Lanka, compared with 5.52 (0.82-11.48) in Sweden, 6.46 (0.00-14.49) in Australia and 12.13 (4.95-21.82) in Canada. Frontier analyses showed that Mesoamerican countries had significantly higher CKD DALY rates relative to other countries with comparable sociodemographic development.
Conclusions: Our results demonstrate that the global toll of CKD attributable to ambient air pollution is significant and identify several endemic geographies where air pollution may be a significant driver of CKD burden. Air pollution may need to be considered in the discussion of the global epidemiology of CKD.
Keywords: chronic renal failure; nephrology; public health.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical