

Dilated cardiomyopathy
- PMID: 31073128
- PMCID: PMC7096917
- DOI: 10.1038/s41572-019-0084-1
Dilated cardiomyopathy
Abstract
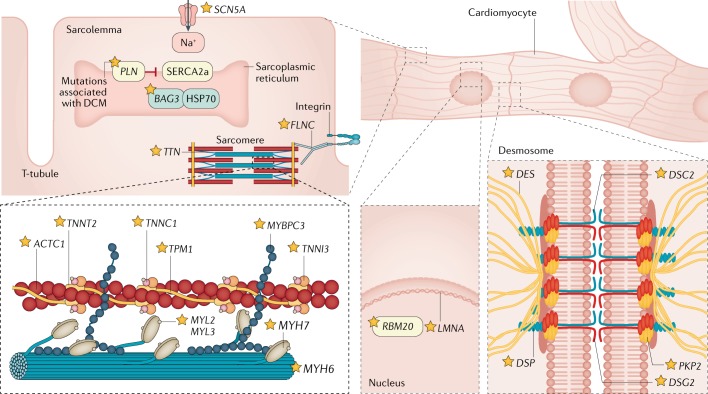
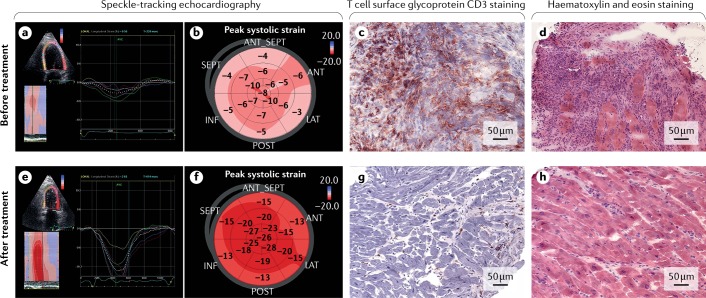
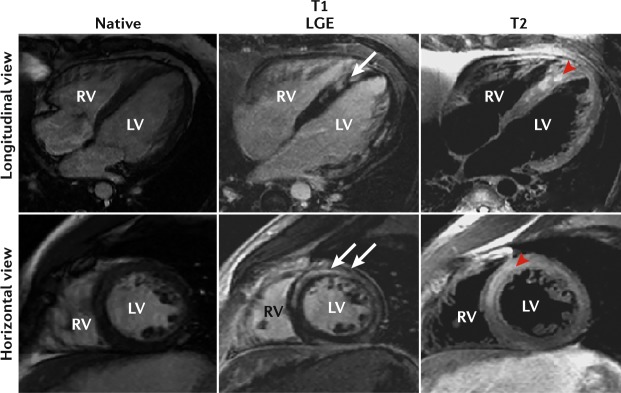
Dilated cardiomyopathy (DCM) is a clinical diagnosis characterized by left ventricular or biventricular dilation and impaired contraction that is not explained by abnormal loading conditions (for example, hypertension and valvular heart disease) or coronary artery disease. Mutations in several genes can cause DCM, including genes encoding structural components of the sarcomere and desmosome. Nongenetic forms of DCM can result from different aetiologies, including inflammation of the myocardium due to an infection (mostly viral); exposure to drugs, toxins or allergens; and systemic endocrine or autoimmune diseases. The heterogeneous aetiology and clinical presentation of DCM make a correct and timely diagnosis challenging. Echocardiography and other imaging techniques are required to assess ventricular dysfunction and adverse myocardial remodelling, and immunological and histological analyses of an endomyocardial biopsy sample are indicated when inflammation or infection is suspected. As DCM eventually leads to impaired contractility, standard approaches to prevent or treat heart failure are the first-line treatment for patients with DCM. Cardiac resynchronization therapy and implantable cardioverter-defibrillators may be required to prevent life-threatening arrhythmias. In addition, identifying the probable cause of DCM helps tailor specific therapies to improve prognosis. An improved aetiology-driven personalized approach to clinical care will benefit patients with DCM, as will new diagnostic tools, such as serum biomarkers, that enable early diagnosis and treatment.
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Maron BJ. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association scientific statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
