

Allogeneic hematopoietic cell transplantation compared to chemotherapy consolidation in older acute myeloid leukemia (AML) patients 60-75 years in first complete remission (CR1): an alliance (A151509), SWOG, ECOG-ACRIN, and CIBMTR study
- PMID: 31073153
- PMCID: PMC6842042
- DOI: 10.1038/s41375-019-0477-x
Allogeneic hematopoietic cell transplantation compared to chemotherapy consolidation in older acute myeloid leukemia (AML) patients 60-75 years in first complete remission (CR1): an alliance (A151509), SWOG, ECOG-ACRIN, and CIBMTR study
Abstract
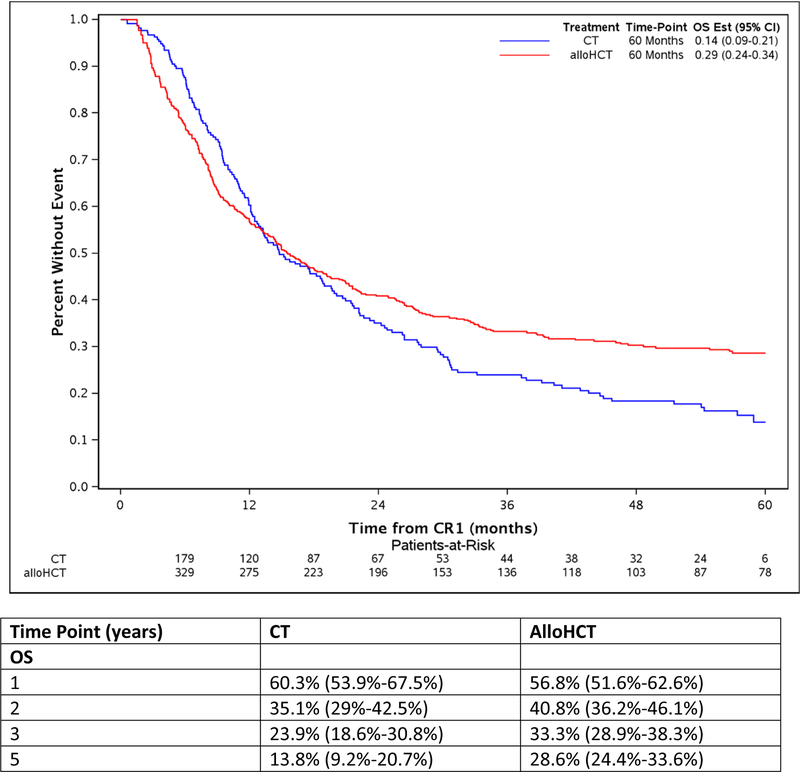
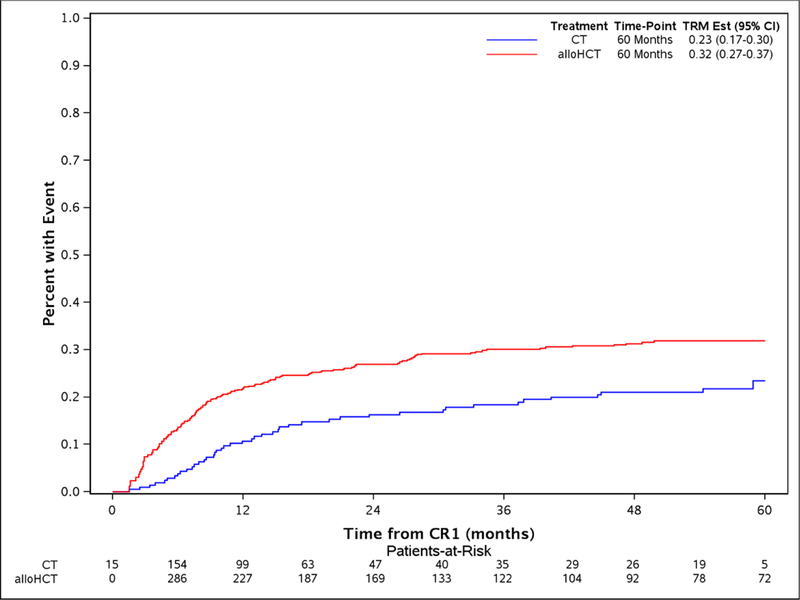
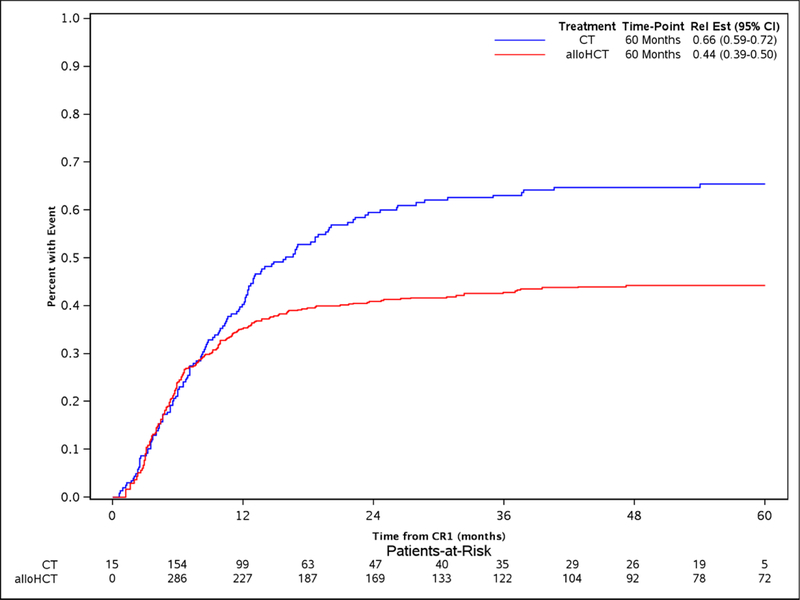
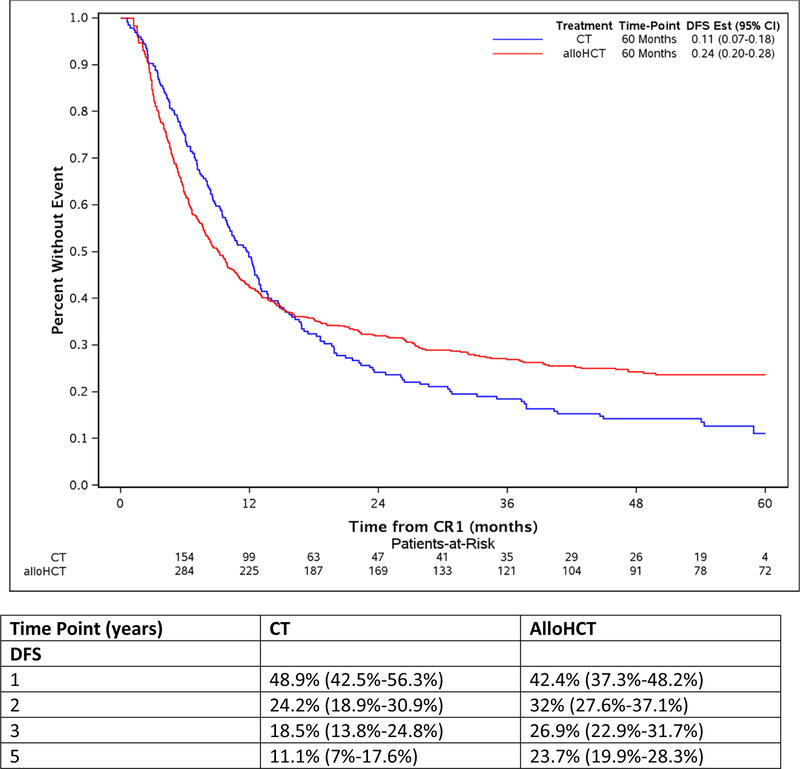
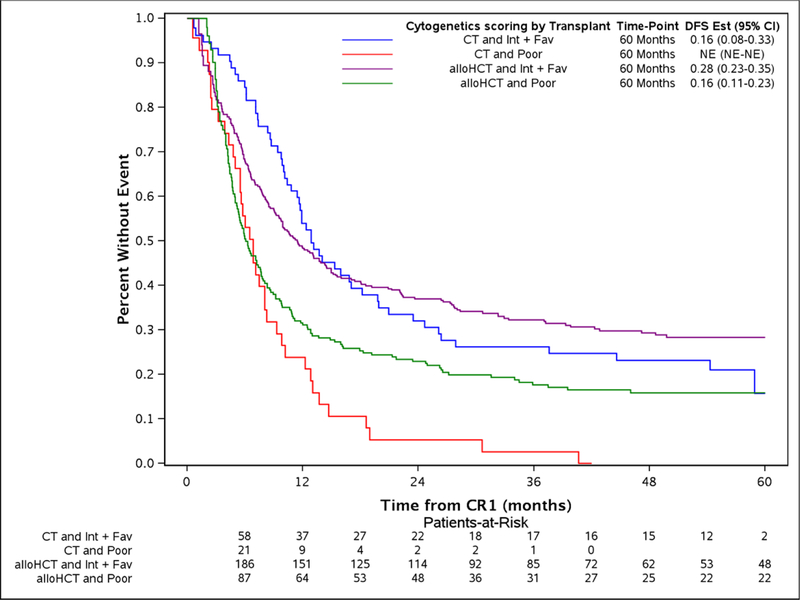
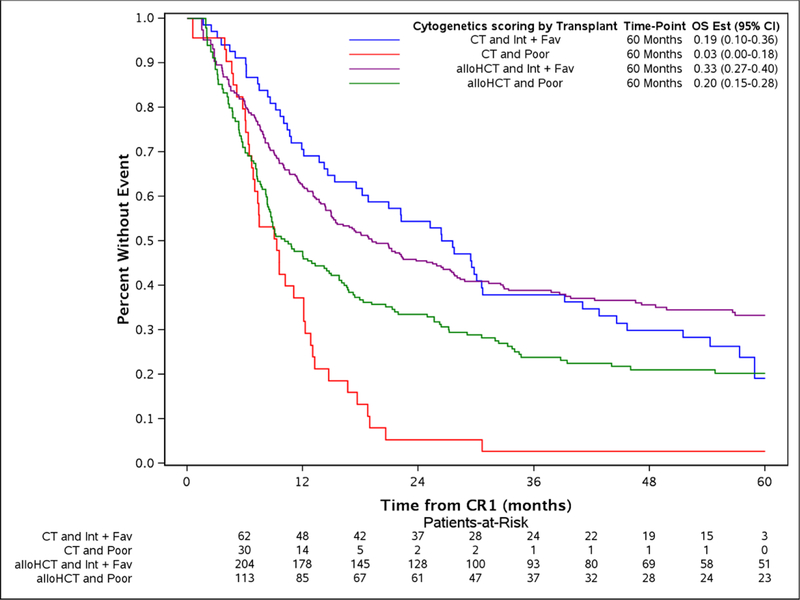
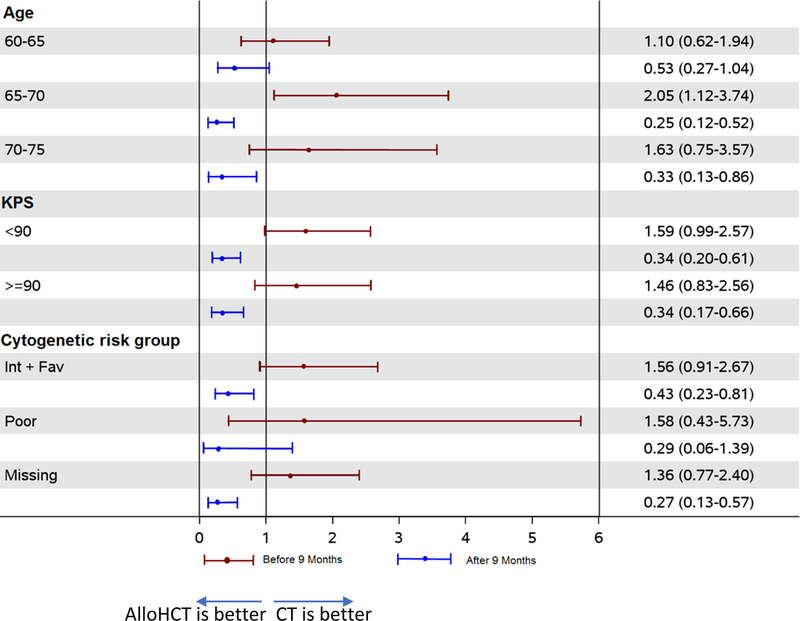
The preferred post-remission therapy for older patients with acute myeloid leukemia (AML) in first complete remission (CR1) remains uncertain. In this retrospective, multicenter study, we compared the outcomes for older AML patients (age 60-77 years) receiving allogeneic hematopoietic cell transplantation (alloHCT) (n = 431) with those treated on prospective National Clinical Trials Network induction and nontransplantation chemotherapy (CT) consolidation trials (n = 211). AlloHCT patients were younger (median age: 64.2 versus 67.9 years, p < 0.001), but more frequently had high-risk AML (high WBC, secondary AML, and unfavorable cytogenetics). Overall survival (OS) was worse in alloHCT during the first 9 months after CR1 (HR = 1.52, p = 0.02), but was significantly better thereafter (HR = 0.53, p < 0.0001) relative to CT. Treatment-related mortality (TRM) following HCT was worse in the first 9 months (HR = 2.8, 95% CI: 1.5-5.2, p = 0.0009), while post-HCT relapse was significantly less frequent beyond 9 months (HR = 0.42, 95% CI: 0.29-0.61, p < 0.0001). Despite higher early TRM, alloHCT recipients had superior long-term OS [29% (24-34%) versus CT 13.8% (9-21%) at 5 years]. Although this is a retrospective analysis with potential biases, it indicates that alloHCT led to heightened early risks from TRM, yet reduced relapse and superior long-term survival relative to CT in older AML patients in CR1.
Conflict of interest statement
Figures
References
-
- O’Donnell MR, Abboud CN, Altman J, Appelbaum FR, Arber DA, Attar E, et al. Acute myeloid leukemia. J Natl Compr Canc Netw 2012. August; 10(8): 984–1021. - PubMed
-
- Kantarjian H, O’Brien S, Cortes J, Giles F, Faderl S, Jabbour E, et al. Results of intensive chemotherapy in 998 patients age 65 years or older with acute myeloid leukemia or high-risk myelodysplastic syndrome: predictive prognostic models for outcome. Cancer 2006. March 1; 106(5): 1090–1098. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA180795/CA/NCI NIH HHS/United States
- U10 CA180836/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- UG1 CA189823/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180819/CA/NCI NIH HHS/United States
- UG1 CA233339/CA/NCI NIH HHS/United States
- UG1 CA233290/CA/NCI NIH HHS/United States
- UG1 CA233331/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U10 CA180791/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- P30 CA033572/CA/NCI NIH HHS/United States
- U10 CA180833/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180838/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
