

Innovations in the Assessment of Primary and Secondary Raynaud's Phenomenon
- PMID: 31073287
- PMCID: PMC6495407
- DOI: 10.3389/fphar.2019.00360
Innovations in the Assessment of Primary and Secondary Raynaud's Phenomenon
Abstract
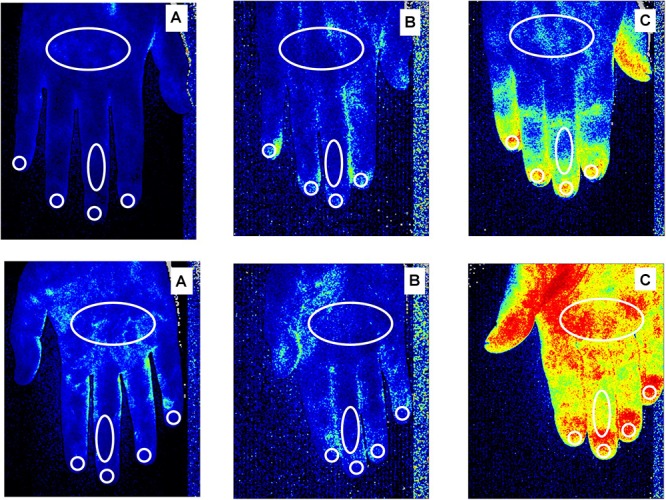
Objectives: Raynaud's phenomenon (RP) is characterized by intense vasospasm of the digital arteries that causes characteristic color changes in fingers. There are two main types of RP: Primary RP (PRP) and Secondary RP (SRP). PRP is a benign condition. Whilst SRP is associated with several connective tissue diseases (CTD), in particular systemic sclerosis (SSc). The objectives of this report were: to present a short review on morphological (nailfold videocapillaroscopy, NVC) and functional techniques (laser tools and thermography) that allow for a correct diagnosis and treatment of RP and to investigate blood perfusion (BP) by laser speckle contrast analysis (LASCA) in different skin areas of hands and face in PRP, SRP to SSc, and healthy subjects (CNT). Methods: 31 PRP patients (LeRoy criteria), 70 SRP to SSc (ACR/EULAR criteria) and 68 CNT were enrolled. BP was assessed by LASCA at the level different areas of hands and face. NVC was performed to distinguish between PRP and SRP, and to detect the proper pattern of nailfold microangiopathy in SSc patients. Results: Both PRP and SRP showed a statistically significant lower BP than CNT at the level of fingertips (p < 0.0001), periungual (p < 0.0001), palmar aspect of 3rd finger (p < 0.0001), and palm areas (p < 0.0001). Moreover, BP was significantly lower in PRP than in SRP to SSc with the "Early" pattern of microangiopathy in the same areas as above (p < 0.04). Conclusion: By considering a small cohort of patients, BP of hands was found lower in PRP than in SSc patients with the "Early" NVC pattern of microangiopathy.
Keywords: Raynaud’s phenomenon; laser techniques; microvascular damage; nailfold videocapillaroscopy; peripheral blood perfusion; systemic sclerosis.
Figures
References
-
- Aschwanden M., Daikeler T., Jaeger K. A., Thalhammer C., Gratwohl A., Matucci-Cerinic M., et al. (2008). Rapid improvement of nailfold capillaroscopy after intense immunosuppression for systemic sclerosis and mixed tissue disease. Ann. Rheum. Dis. 67 1057–1059. 10.1136/ard.2007.082008 - DOI - PubMed
-
- Avouac J., Fransen J., Walker U. A., Riccieri V., Smith V., Muller C., et al. (2011). Preliminary criteria for the very early diagnosis of systemic sclerosis: results of a delphi consensus study from EULAR scleroderma trials and research group. Ann. Rheum. Dis. 70 476–481. 10.1136/ard.2010.136929 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials