

Post-colonoscopy colorectal cancer in Belgium: characteristics and influencing factors
- PMID: 31073539
- PMCID: PMC6506335
- DOI: 10.1055/a-0751-2660
Post-colonoscopy colorectal cancer in Belgium: characteristics and influencing factors
Abstract
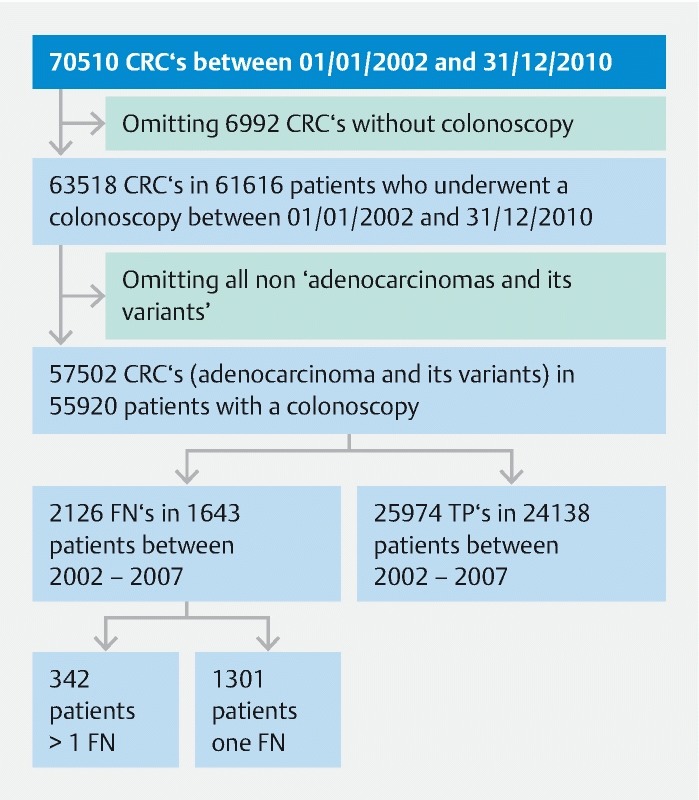
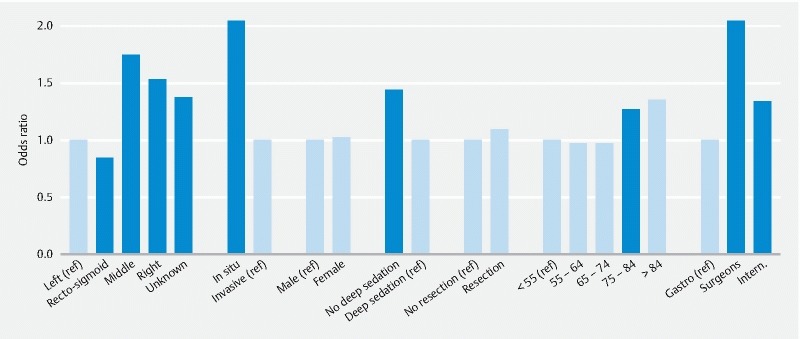
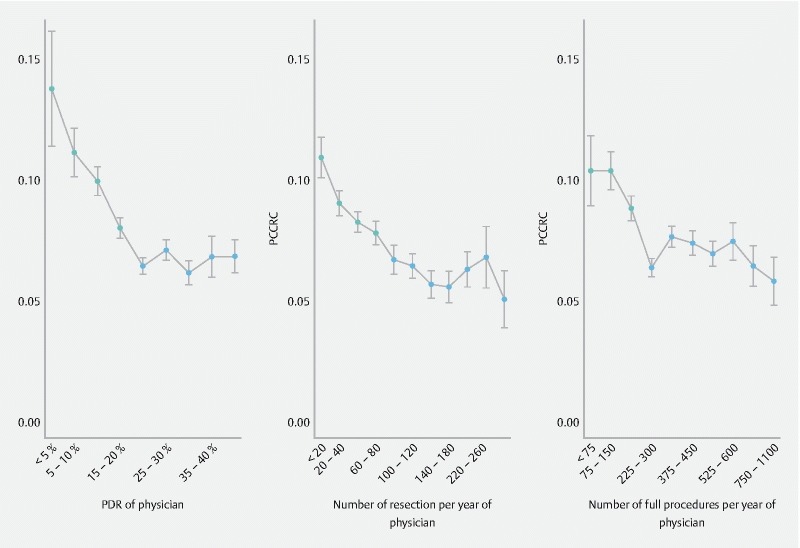
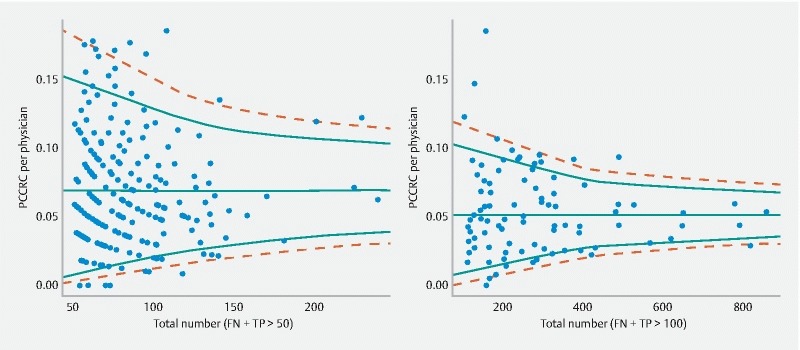
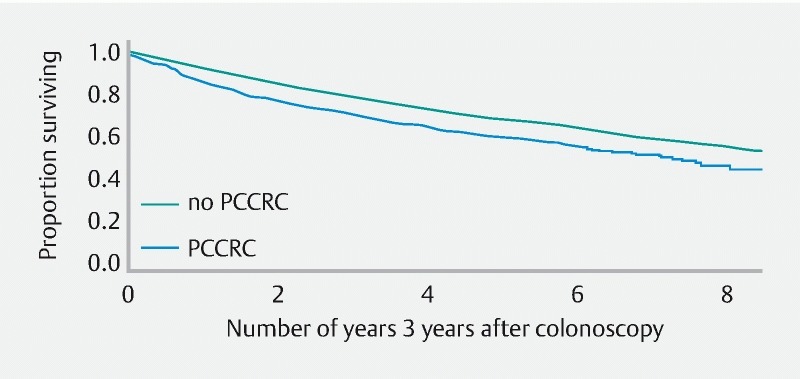
Background and study aims Post-colonoscopy colorectal cancer (PCCRC) is an important quality parameter of colonoscopy. Most studies have shown that the risk for colorectal cancer is reduced after an index colonoscopy for screening or diagnostic purposes with or without polypectomy. In this study, we aimed to quantify and describe PCCRC in Belgium, including the possible relationships with patient, physician, and colonoscopy characteristics. Patients and methods Reimbursement data on colorectal related medical procedures from the Intermutualistic Agency (IMA-AIM) were linked with data on clinical and pathological staging of colorectal cancer (CRC) available at the Belgian Cancer Registry (BCR) over a period covering 9 years (2002 - 2010). Results In total, 63 518 colorectal cancers were identified in 61 616 patients between 2002 and 2010. We calculated a mean PCCRC rate of 7.6 %. PCCRC was significantly higher in older people and correlated significantly with polyp detection rate and the number of resections and procedures performed per year per physician. Conditional observed survival, given still alive 3 years since first colonoscopy, for PCCRC was worse than for CRC. Older patients and patients with invasive carcinomas had a worse outcome. Conclusions Although no quality register exists in Belgium, we were able to demonstrate that PCCRC in Belgium is directly related to the experience of the physician performing the procedure. In the absence of a quality register, utilization of population-based data sources proved to be a valuable tool to identify quality parameters.
Conflict of interest statement
Figures
References
-
- Winawer S J, Zauber A G, Ho M N et al.Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. NEJM. 1993;329:1977–1981. - PubMed
-
- Brenner H, Chang-Claude J, Seiler C M et al.Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med. 2011;154:22–30. - PubMed
LinkOut - more resources
Full Text Sources